Embed Size (px)
Citation preview
E n q u 6 t e sur la d 6 s i n f e c t i o n des e n d o s c o p e s dans 2 3 d 6 p a r t e m e n t s f r a n ~ a i s
G. DAUMY IFFA CREDO, L'Arbresle (France)
Enquiry on the disinfection of endoscopes in 23 french ,, d6partements ,,
Encuesta sobre la desinfecci6n de endoscopios en 23 departementos franceses
RI~SUMI~
Une enqu6te sur les pratiques de nettoyage et d6sinfection des endoscopes a 6t6 r6alis6e dans 23 d6partements franqais par interrogatoire de 171 personnes exerqant dans une unit6 d'endoscopie de 55 h6pitaux et 19 cliniques en 1987. I1 en ressort que 65 % des unit6s ne poss6dent pas de protocole d6fini pour l 'entretien du mat6riel, et que la chronologie des diverses op6rations avec respect des temps n6cessaires ~ Faction des produits n'est respect6e que dans 20 % des cas environ. Un effort de formation du personnel de ces unit6s apparait indispensable.
SUMMARY
This paper deals with a survey on the cleaning and disinfection procedures performed during 1987 in 23 french departements by interrogation of 171 professionals working in an endoscopic unit of 55 public hospitals and 19 private hospitals. The results show that 65 % of the units do not follow a stirtly defined protocol and that only about 20 % respect the time intervals necessary for a complete action of the products. Thus an effort of education seems useful.
RESUMEN
Se realiz6 una encuesta en 23 Departamentos franceses sobre las prticticas de limpieza y desinfecci6n de endoscopios, por medio de un interrogatorio a 171 personas que trabajaban en una Unidad de Endoscopia de 55 Hospitales y 19 Clinicas. El traba/o fu~ realizado en 1987. Se obtiene la conclusi6n de que un 65 % de Unidades no tienen un protocolo definido para mantenimiento de su material, y que la cronologia de las diversas operaciones de limpieza respecto del tiempo necesario para la actuaci6n correcta de los productos de desinfecci6n empleados no es respetada sino en un 20 % de casos aproximadamente. Parece indispensable realizar un esfuerzo para formar adecuadamente al personal de dichas Unidades.
INTR OD UCTION
Dans le cadre des missions d'un agent technico- commercial, la pr6sentation aux professionnels de la sant6 des produits et des m6thodes pour le nettoyage et la d6sinfection de l'ensemble du mat6riel d'exploration fonctionnelle conduit h la constatation de l'existence :
- - d ' u n e barri6re repr6sent6e par I'usage d'un vocabulaire off les termes n'ont pas la m6me signi- fication pour tous;
- - d e s pratiques tr6s diff6rentes dont certaines conduisent a s'interroger sur leur justification.
Or, pourtant, I'AFNOR (norme NF T-72101) a mis en place une terminologie ; l'usage hospitalier a consacr6 des op6rations techniques de d6conta- mination (= pr6d6sinfection), nettoyage et d6sin- fection, et des machines et produits cibl6s sont largement r6pandus.
C'est pourquoi nous avons r6alis6 une enqu6te sur les faqons de proc6der pour l'entretien du mat6riel d'endoscopie dans la zone g6ographique
Tir6s h part : G. DAUMY, IFFA CREDO, 69210 L'Arbresle (France).
Mots-cl~s: d6sinfection, endoscopie, enqu6te.
Key words : disinfection, endoscopy, enquiry.
Palabras clave : disinfecci6n, encuesta, endoscopia.
Acta Endoscopica Volume 19 - N ~ 3 - 1989 205
couverte par notre activit6, en milieu hospitalier priv6 et public. La m6thodologie, les r6sultats et les enseignements h tirer de cette enqu6te sont pr6sent6s darts cet article dont le but est d'amener une sensibilisation ~ un usage plus homog~ne de la terminologie et des m6thodes et produits disponi- bles.
PRESENTATION DE L'ENQUI~TE
Cette enqu6te s'est d6roul6e sur la p6riode allant de mars ~ juin 1987. Afin d'obtenir une
certaine pr6cision dans la saisie des donn6es, un premier questionnaire a 6t6 6tabli, suivi de sa phase exp6rimentale de validation. C'est h la suite du d6pouillement de ces premieres r6ponses que le questionnaire pr6sent6 en annexe 1 a 6t6 adopt6 d6finitivement et exploit6. Le questionnaire a 6t6 pr6sent6 dans tous les 6tablissements et cabinets m6dicaux visit6s dans le Sud-Ouest de la France (fig. 1 ) .
Dans l'6chantillon sont uniquement prises en compte les r6ponses des personnes travaillant et/ ou utilisant du mat6riel d'endoscopie requ6rant l'asepsie la plus rigoureuse, qui ont toutes 6t6
NOUVEAU OiCOUPAG[ ~ l l lC I i lS DiPAITEIENT$
ti SEINE I SEINI I Ol l l
HAUT$ . Ot - SEINE
Sl~ l~ . SAINt T)[N|$
/sl$ ', El oriel,
de Co/cos { --. ,/ 4.r
X--X. ', N o r d ~ i # * ' s0=~e "" . . . . "-...,- . . . . . . . I J'
' t A/she ' - - - ~ - i / Ri~oen#Mi ~ & O ~ f i e / i t / m e f"" " - - . . . . 4
~ o [ I ~ ... "~ o~,e '~ .J_.. ! ,..--, ,,, \ ~ ~ " < ' ..... ~ ', ( ....... .<",~e,,. ~ ',,_ " " - + " . . . I
" * ~ ) u ~:~ Ce/vidos \ Euee ~ " ,i M l e n e ~ , ,, l O l i / l e . . . . . . ' - - ' ~ I$~lnC.lrl i . . . . o h i , . , i ~ , . t , , ~ / . , ~ ) .. , , t " - - . �9 a . R/ , ,n.M
. - , " 1 . l ' , - - - - _ - - " ', l~ I ~ . ~ . ; - - ' , , ~ e . n ~ . ; d I ' i' " ' . " - . / - , . . . . . " ~' . ~ , " ' - - % ~ . . . . . n rn . . . . . . . . "., L k d l . .- -, . . . . n,vo.~ene .. , r I
�9 - i ~. ~ 11 "_i "~ - - ",, ,' [ ' ~ - I t : , �9 ". , "'-.,.' ~ I ~rw "; ~ . / * " t . e ~ i ' % M �9 , ., Eure ; �9 " - . I ~- , ', " - ' / / : -~ ,~ ~ . . - - . ' a . ~ . . - - ~ - 4 . - - ' ~ , - . ~ J I / . . . . . . . . . r " - . . . ' " , .- . . . . . I + I No/'d " C~tes duNo/'d / ~l ie ~* F " " ~ . " '~eg Lo~r ~ ~et Marne ~ Aube ' , H l u ~ e ~ "r;. . . . . . ~-, I /
' �9 " " "u-----n- ~ " �9 �9 ~ ( ' " "" ", . * ~ VO$ge.S " "" 1' i / - . . l .a zrn ~ , " " ', , l l i p n - , " , . . . . . - - , w / e , . ( r ,.. , . . , . y ' - } _ ~ . ~ �9 ~ :~e.t 'q
. I " ' . q C ' 4 . ~ i S a r t h e , ' . _ ~ , . ~ I ",. : ' " ', - ,' - - : - T iud ~v~ J ~ j 10 r ,~ . . I LOI r '~ I Yonne ' - . , 4 - , . - - . . . _ , ~rnon I
~ " ~ o ~ . . " / . - ~' ; ' . ~ ( ,', "-. ,-' " . . ~ :~--. , . . . - r - - - - . . , / t o m er �9 # I t I 3cone ' I +
~ P ' " , " " " ' , . . . . . . . ", Chee . / " " - - s _ . ~ = b ~ - ~ . - ~ . . . . L o . ., . . , . . ,. . . . . . . , ' " ' ~ - - - . . . . _ $ - - . ...... : . . . . . . . . . - - . ~ . i r . / ' ~ w / . ". , 7 . ~ ~ �9 11 . . I [,Ot,~ O UP / , I ~
- - =If AUint4que " - l e t Lome ,, ,no~e ; �9 �9 "- , . �9 ' .~ / " ~, L3 ~ ~ : . . . . :' e~o , . ' , . , _ J " c~e~ \ " t : ' G O o ~ , ,~"
- �9 ~a ',, , ' ~ " ~ " , - ! N~ev~,e 5 . / ' l =
) ' " " ' 1 ( ~ ~ ' " " Oeux ' ", .',Se6ne er Loire; du~o ~ /~ X Ve.,,e V,e.., =.~ ( ~ ,., ,, , .. ~ 3dv, ,u }
T Cl'euse �9 ' . - - - . t ,"RhOne" i HauCe Sovoie.~.
I /r ~ . I ' J v = u ~ D T - - - , j - , . , . T ~
. - x I . J "o | " , , . o . r �9 ~eVO/O %
" , " " - - ' " ~ , ' ~ 1 r ~ . , O o r d o g ~ e l d _ , _ . . , , / , , . , ~
I - , , ~ , ContW ,MeuteLo/Pe / ~ t . . 4 " - ~
I . . : , , ~ . 2 ) O r ~ m ~ " x . " - " llautes~% 01rondo t_., ; / . . ,' h I -~ . ~ / " A N ~ c h e , - - - " ~ l . .
. . ~ , " LOr / " / ~, ~ . . ' ~ ' I "c~ / J . . . . . . . , / " V - - - ' ~ L o z e r e ' ' ' ; Iz
, - - r " !l �9 " , / , - , ' . . / I ( ' , - - , / LOr e t ,', . , ~ Avev~on I ~ ; , , , , . " , - " " J " ' - . . , ! Garonne . ' l . r v ~I ( ~ . , / , . - . f ~ , . i - - - ~ " . . , ,., , / ~ , ~
p ' - ~ ~ . . . . . . . . " ' ~ L ~, " ~ , , " . , ' J "~ A l p e s i - - " ~ " ' " ' : ~ T i r n ~ . , . ~ o - ~ " ' y - - . " - ~ ~. __ ~ v a u c l u s ~ _ d~/,oe.t + + ~
Lendes "--J ~ r - - " ~ , u a l ~ , , , o e H~ur.e " - u �9 . - / u a / ' o n n e L % "~ , i . ~ l l I M l # m e s
-, ~ ' " ' " " " ; �9 Ta~n l . . , " / - ; , / "~ r~ovence j
" " ' " ' " . . . . / . . . . . ' " " " " ' " ' " \ l ' ' l ' a r . . . . . . . . . . �9 . - ~ , . ~ , ' ~ ' * ,.',. i _ ~ , . , , ~ 4 ~ . , / . , ~ ,; _ . , ; _ ~ ' . ~ . . ' : . . : . ~ . . . ~ ;
,,.'~ " " , - ~ , ' - i . . . . . " - / ' - - U 7 - - l i , f - c ~ - I j r , , Py~nee$ :~:ltau~e,l/ (-:: : " ( . , Aude " " ~ I ~ ~ , . . t ~ *V_
Figure 1
Carte geographique des etabtissements visites pour renqu6te .
Geographical map of the units visited for the inquiry.
206 V o l u m e 1 9 - N ~ 3 - 1 9 8 9 Acta Endoscopica
interrog6es par le m6me enqu6teur, afin qu'aucun biais ne puisse 6tre introduit. Le choix des mots, (d6termin6s ~ la premiere enqu6te), est laiss6 ~ la personne interrog6e. Jamais elle ne sera guid6e ou influenc6e. Avant toute audition, l'autorisation est demand6e d'abord ~ la direction hi6rarchique, puis
la personne elle-m6me. Elle 6tait donc toujours libre de sa participation, et cela sans t6moin, faci- litant l'acceptation de l'entretien. Afin d'6tre bien comprise, la question principale (n ~ 4), 6tait au minimum r6p6t6e deux lois.
Dans la phase exp6rimentale de l'enquSte, tous les services pratiquant des explorations fonction- nelles ont 6t6 interrog6s, mais devant les r6ponses recueillies, le champ d'investigation a 6t6 limit6 au seul mat6riel d'endoscopie p6n6trant dans un site d6termin6 de l'organisme, o/l en raison des risques de contamination existant, l'asepsie la plus rigou- reuse est exig6e. La chronologie demand6e d6bu- tait au moment o/~ l'endoscope est retir6 d'un patient, pour ensuite 6tre r6utilis6 sur un autre patient en attente. Une lois la r6ponse not6e, celle-ci a 6t6 relue imm6diatement, afin que la personne interrog6e soit parfaitement d'accord, 6vitant ainsi les erreurs de saisie qui pourraient fausser la pr6cision de l'enqu6te.
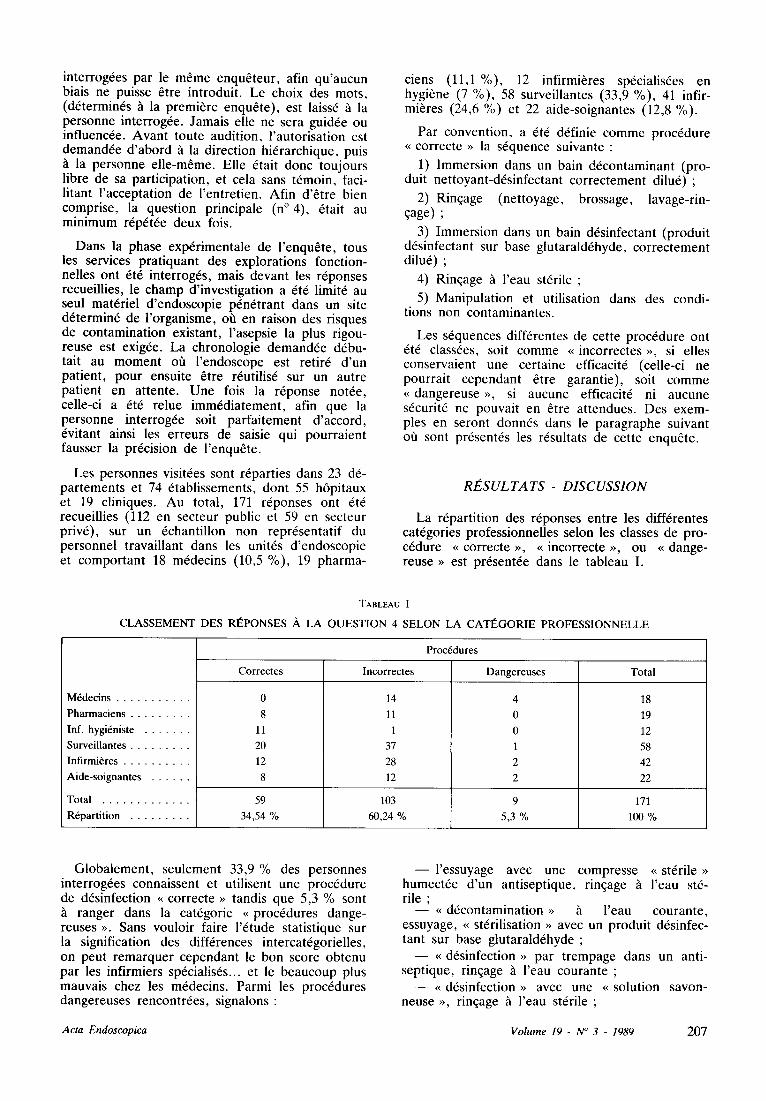
Les personnes visit6es sont r6parties dans 23 d6- partements et 74 6tablissements, dont 55 h6pitaux et 19 cliniques. Au total, 171 r6ponses ont 6t6 recueillies (112 en secteur public et 59 en secteur priv6), sur un 6chantillon non repr6sentatif du personnel travaillant dans les unit6s d'endoscopie et comportant 18 m6decins (10,5 %), 19 pharma-
ciens (11,1%), 12 infirmi~res sp6cialis6es en hygiene (7 %), 58 surveillantes (33,9 %), 41 infir- mitres (24,6 %) et 22 aide-soignantes (12,8 %).
Par convention, a 6t6 d6finie comme proc6dure <~ correcte >> la s6quence suivante :
1) Immersion dans un bain d6contaminant (pro- duit nettoyant-d6sinfectant correctement dilu6) ;
2) Rinqage (nettoyage, brossage, lavage-rin- Gage) ;
3) Immersion dans un bain d6sinfectant (produit d6sinfectant sur base glutarald6hyde, correctement dilu6) ;
4) Rinqage h l'eau st6rile ;
5) Manipulation et utilisation dans des condi- tions non contaminantes.
Les s6quences diff6rentes de cette proc6dure ont 6t6 class6es, soit comme ~ incorrectes ~, si elles conservaient une certaine efficacit6 (celle-ci ne pourrait cependant 6tre garantie), soit comme ,, dangereuse ,,, si aucune efficacit6 ni aucune s6curit6 ne pouvait en 6tre attendues. Des exem- pies en seront donn6s dans le paragraphe suivant of~ sont pr6sent6s les r6sultats de cette enqu6te.
R t E S U L T A T S - D I S C U S S I O N
La r6partition des r6ponses entre les diff6rentes cat6gories professionnelles selon les classes de pro- c6dure ~ correcte >~, ~ incorrecte ~, ou ,~ dange- reuse >~ est pr6sent6e dans le tableau I.
TABLEAU I
CLASSEMENT DES RI~PONSES A LA QUESTION 4 SELON LA CATI~GORIE PROFESSIONNELLE
M6decins
Pharmaciens
Inf. hygi6niste
SurveiUantes
Infirmi~res
Aide-soignantes
Total
R6partition
Proc6dures
Correctes Incorrectes Dangereuses Total
0
8
11
20
12
8
14
11
1
37
28
12
18
19
12
58
42
22
59 103 9 171
34,54 % 60,24 % 5,3 % 100 %
Globalement, seulement 33,9 % des personnes interrog6es connaissent et utilisent une proc6dure de d6sinfection ,~ correcte ~ tandis que 5,3 % sont
ranger dans la cat6gorie ~< proc6dures dange- reuses ~. Sans vouloir faire l'6tude statistique sur la signification des diff6rences intercat6gorielles, on peut remarquer cependant le bon score obtenu par les infirmiers sp6cialis6s.., et le beaucoup plus mauvais chez les m6decins. Parmi les proc6dures dangereuses rencontr6es, signalons :
- - I ' e s suyage avec une compresse ~ st6rile >> humect6e d'un antiseptique, rin~age ~ l'eau st6- rile ;
- - ~ d6contamination >~ h l'eau courante, essuyage, ~ st6rilisation ~ avec un produit d6sinfec- tant sur base glutarald6hyde ;
- - <~ d6sinfection ~ par trempage dans un anti- septique, rinqage ~ l'eau courante ;
--<~ d6sinfection ~ avec une <~ solution savon- neuse ~>, rin~age ~t l'eau st6rile ;
A c t a E n d o s c o p i c a V o l u m e 19 - N ~ 3 - 1989 207
- - l avage ~ I'eau courante, essuyage avec une compresse et ~ st6rilisation ~ avec une pastille de formol.
Les termes techniques utilis6s par les personnes interrog6es montrent une assez grande m6connais- sance des concepts de nettoyage, d6contamination, d6sinfection, st6rilisation. En particulier 23 per- sonnes (13,5 %) pensent que les endoscopes sont st6riles, alors qu'en r6alit6, seulement 2 % du mat6riel l'6tait (et encore seulement h la sortie de l'appareil), car st6rilis6 ~t l'oxyde d'6thyl6ne.
A la question n~ concernant l'existence d'un protocole dans l'unit6 pour rentretien du mat6riel d'endoscopie, une r6ponse positive n'est obtenue que dans 35 % des cas. Dans les faits, seulement 21% des personnes ont pu fournir un protocole 6crit, mais dans 47 % des cas ce protoeole n'6tait pas actualis6 avec les produits disponibles. La con- naissance des produits disponibles est bonne chez les infirmi6res sp6cialis6es (92 %), mais 6tonnam- ment basse chez les utilisateurs (pharmaeiens 63 %, surveillantes 55 %, ASH 41%) pour ne pas parler des m6decins (11%) ! De m6me, seulement 18 % des personnes interrog6es connaissent la dif- f6rence entre les objectifs et les moyens des op6- rations de d6contamination (ou pr6d6sinfection ou d6sinfection initiale) et de d6sinfection.
L'6tude du temps consacr6 h l'ensemble des op6rations de d6contamination, nettoyage et d6sin- fection du mat6riel entre deux patients est r6v61a- trice des probl~mes rencontr6s pour l'application correcte de la s6quence puisque le temps consid6r6 comme n6cessaire et suffisant de 30 minutes n'est respect6 que dans 30 % des cas. Les autres dur6es s'6chelonnant entre 5 minutes (15 %), 10 minutes (27 %) et 20 minutes (28 %), il est probable que dans la pratique, la dur6e soit encore plus courte.
On peut enfin signaler que dans 6 % des cas, nous avons retrouv6 l'usage de pastilles de trioxy- m6thyl6ne ou autre produit h base de formald6- hyde pour ~, st6riliser ~, le mat6riel, ce qui est une pratique potentiellement tr6s dangereuse en raison de la toxicit6 de cette mol6cule qui va se d6poser sur le mat6riel et ne sera pas 61imin6e par rin~age
l'eau.
C O N C L U S I O N
Cette 6tude sur un 6chantillon qui n'a aucune pr6tention h la repr6sentativit6 des unit6s d'endoscopie, permet de constater que 65 % des proc6dures utilis6es pour l'entretien du mat6riel sont & consid6rer comme incorrectes ou dange- reuses, 65 % des unit6s ne poss6dent pas de pro- tocole d6fini, et que la chronologie des op6rations n'est respect6e que dans 20 % des cas environ. Le pourcentage de patients ne courant aucun risque de contamination lors des examens est faible, mais heureusement ces patients dans l'immense majorit6 des cas poss~dent des d6fenses immunitaires satis- faisantes pour 61iminer l'6ventuel contaminant.
La situation doit cependant 6tre am61ior6e, car si le risque infectieux n'est ni majeur, ni omnipre- sent dans ces diverses sp6cialit6s de l'exploration endoscopique, le patient est en droit d'attendre que les pr6cautions de d6sinfection n6cessaires a~ent 6t6 prises.., si l'on veut 6viter des campagnes de presse analogues ~ celle rencontr6e avec l'acu- puncture. II convient donc que chaque unit6 d'endoscopie se dote d'un protocole, des produits et du mat6riel n6cessaire ~ son application. Ceci ne sera obtenu que par la mise en place d'une formation du personnel et d'une information des responsables.
208 V o l u m e 19 - N ~ 3 - 1989 Acta Endoscop ica
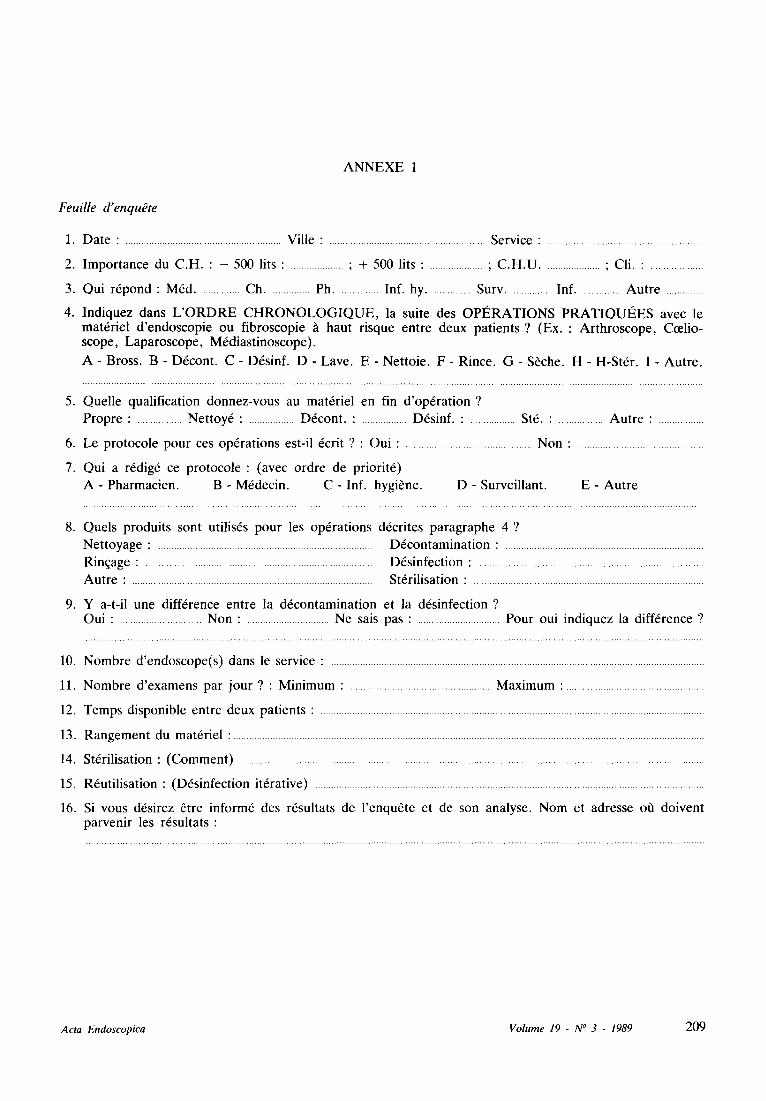
A N N E X E 1
Feuille d'enqu~te
1. D a t e : ........................................................... V i l l e : ........................................................... S e r v i c e : ...........................................................
2. I m p o r t a n c e d u C . H . : - 5 0 0 l i t s : .................... ; + 5 0 0 l i t s : .................... ; C . H . U ..................... ; C l i . : ....................
3. Q u i r 6 p o n d : M 6 d ............... C h ............... P h ............... I n f . h y ............... S u r v ............... I n f ............... A u t r e ..............
4. I n d i q u e z d a n s L ' O R D R E C H R O N O L O G I Q U E , la s u i t e d e s O P I ~ R A T I O N S P R A T I Q U I ~ E S a v e c l e m a t 6 r i e l d ' e n d o s c o p i e o u f i b r o s c o p i e ~ h a u t r i s q u e e n t r e d e u x p a t i e n t s ? ( E x . : A r t h r o s c o p e , C e e l i o - s c o p e , L a p a r o s c o p e , M 6 d i a s t i n o s c o p e ) .
A - B r o s s . B - D 6 c o n t . C - D 6 s i n f . D - L a v e . E - N e t t o i e . F - R i n c e . G - S ~ c h e . H - H - S t 6 r . I - A u t r e .
5. Q u e l l e q u a l i f i c a t i o n d o n n e z - v o u s a u m a t 6 r i e l e n f i n d ' o p 6 r a t i o n ?
P r o p r e : ................. N e t t o y 6 : ................. D 6 c o n t . : ................. D 6 s i n f . : ................. S t6 . : ................. A u t r e : .................
6. L e p r o t o c o l e p o u r c e s o p 6 r a t i o n s e s t - i l 6 c r i t ? : O u i : ................................................ N o n : ................................................
7. Q u i a r 6 d i g 6 ce p r o t o c o l e : ( a v e c o r d r e d e p r i o r i t 6 )
A - P h a r m a c i e n . B - M 6 d e c i n . C - I n f . h y g i b n e . D - S u r v e i l l a n t . E - A u t r e
8. Q u e l s p r o d u i t s s o n t u t i l i s 6 s p o u r l e s o p 6 r a t i o n s d 6 c r i t e s p a r a g r a p h e 4 ?
N e t t o y a g e : ................................................................................. D 6 c o n t a m i n a t i o n : ...........................................................................
R i n q a g e : ...................................................................................... D 6 s i n f e c t i o n : .....................................................................................
A u t r e : ........................................................................................... S t 6 r i l i s a t i o n : .......................................................................................
9. Y a - t - i l u n e d i f f 6 r e n c e e n t r e l a d 6 c o n t a m i n a t i o n e t l a d 6 s i n f e c t i o n ? O u i : ............................... N o n : ............................... N e s a i s p a s : ............................... P o u r o u i i n d i q u e z l a d i f f 6 r e n c e ?
10. N o m b r e d ' e n d o s c o p e ( s ) c l ans le s e r v i c e : .............................................................................................................................................
11. N o m b r e d ' e x a m e n s p a r j o u r ? : M i n i m u m : ..................................................... M a x i m u m : .....................................................
12. T e m p s d i s p o n i b l e e n t r e d e u x p a t i e n t s : .................................................................................................................................................
13. R a n g e m e n t d u m a t 6 r i e l : ..................................................................................................................................................................................
14. S t 6 r i l i s a t i o n : ( C o m m e n t ) ...............................................................................................................................................................................
15. R 6 u t i l i s a t i o n : ( D 6 s i n f e c t i o n i t 6 r a t i v e ) ...................................................................................................................................................
16. Si v o u s d 6 s i r e z 6 t r e i n f o r m 6 d e s r 6 s u l t a t s d e l ' e n q u 6 t e e t d e s o n a n a l y s e . N o m e t a d r e s s e off d o i v e n t p a r v e n i r l e s r 6 s u l t a t s :
A c t a E n d o s c o p i c a V o l u m e 19 - N ~ 3 - 1989 209
INTRODUCTION
Within the scope of the assignments of a techni- cal sales agent, the presentation to professionals in the health world of products and methodes for the cleaning and disinfection of all functional explora- tion equipment, leads to the recording of the exis- tence :
- - of a barrier, in the form of vocabulary where words do not have the same meaning for all parties involved ;
- - o f highly differentiated forms of practice, including some which leave open questions in the field of their justification.
Yet, AFNOR (standard NF-T 72101) has impo- sed a terminology ; hospital practice has institutio- nalized decontamination (= pre-disinfection), clea- ning and disinfection operations, and the related machines and products are widely distributed.
That is why we have completed an enquiry within the geographical area covered by our acti- vity, on the methods used for the maintenance of endoscopic equipment in the public and private hospital environment. The methodology, the results and lessons which can be gained from this enquiry are represented in this article, the object of which is to help to make persons involved more attentive to a more homogeneous use of the terminology, and available methods and products.
PRESENTATION OF THE ENQUIRY
This enquiry has taken place over the period which extends from March to June 1987. In order to obtain a certain accuracy in the input of data, a first questionnaire was established, followed by its experimental validation phase. It is at the outcome of the analysis of these first anwers that the ques- tionnaire presented on Annex 1 was definitively adopted and exploited. The questionnaire was pre- sented in all medical establishments and offices visited throughout the south-western part of France (fig. 1).
In the sample retained, only the answers from persons working with and~or using endoscopic equipment which requires the strictest form of asepsy have been taken into account, in order to avoid the introduction of any form of bias. The choice of words, (determined in the course of the first enquiry), is left to the person being questioned. This person is thus never guided or influenced. Before any interview, authorization is first applied for at the hierarchic management level, then from the person himself. The person was thus always freely taking part, without any witness, thus facilita- ting assent for the interview. In order to be well understood, the main question (n~ was repeated at least twice.
Within the experimental phase of the enquiry, all the departments practicing functional explorations
were interviewed, but in view of the answers collec- ted, the investigation field was limited to only the endoscopic equipment which comes into a determi- ned site within the organization, where (in view of existing contamination risks), the strictest asepsy is required. The required chronology was scheduled to start at the moment where the endoscope is withdrawn from a patient, with the purpose of then being re-used for another waiting patient. Once the answer was written down, it was immediately read out again in order to make sure that the person being interviewed was perfectly in agreement, the purpose being to avoid input errors which could distort the accuracy of the enquiry.
The persons visited are divided out between the 23 ~, d~partements ,~ and 74 establishments, inclu- ding 55 hospitals and 19 clinics. In all, 171 answers were collected, (112 in the public sector and 59 in the private sector) from a non-representative sam- pling of personnel working in the endoscopy units, including 18 doctors (10.5 %), 19 pharmacists (11.1%), 12 nurses specialized in hygiene (7 %), 58 supervisors (33.9 % ), 41 nurses (24.6 %), 22 assistant-nurses (12.8 %).
As was agreed, the following sequence was approved as the ~, correct procedure ~, :
1) Immersion in a decontaminating bath (pro- perly diluted cleaning/ desinfecting product) ;
2) Rinsing (cleaning, brushing, washing~rin- sing) ;
3) Immersion in a desinfecting bath (properly diluted glutaraldehyde base disinfectant) ;
4) Rinsing in sterile water ;
5) Manipulation and use under non-contamina- ting conditions.
The different sequences of this procedure have been classified either as ~ incorrect ~ if they retai- ned a certain efficacy (without any possible form of guarantee at that level), or as ~ dangerous ~, if no efficacy and no safety were to be expected. Exam- ples will be submitted in the following paragraph, where the results of this enquiry are presented.
RESULTS-DISCUSSION
The allotment of answers between the various professional categories in line with : ~ correct ,,, ~ incorrect ~,, or ,~ dangerous ~ procedure classifica- tions is presented in Table L
Globally speaking, only 33.9 % of persons inter- viewed were aware of, and used, a ~ correct ,, disinfection procedure, whereas 5.3 % are to be classified under the ~ dangerous procedures ,~ class. Without attempting to proceed with a statistical study on the significance of the various intra-cate- gory differences, the good score obtained by specia- lized nurses is to be noted.., as well as the much less favourable score amongst doctors. Included within the dangerous procedures which were reco- gnized, the following are to be noted :
210 Volume 19 - N" 3 - 1989 Acta Endoscopica
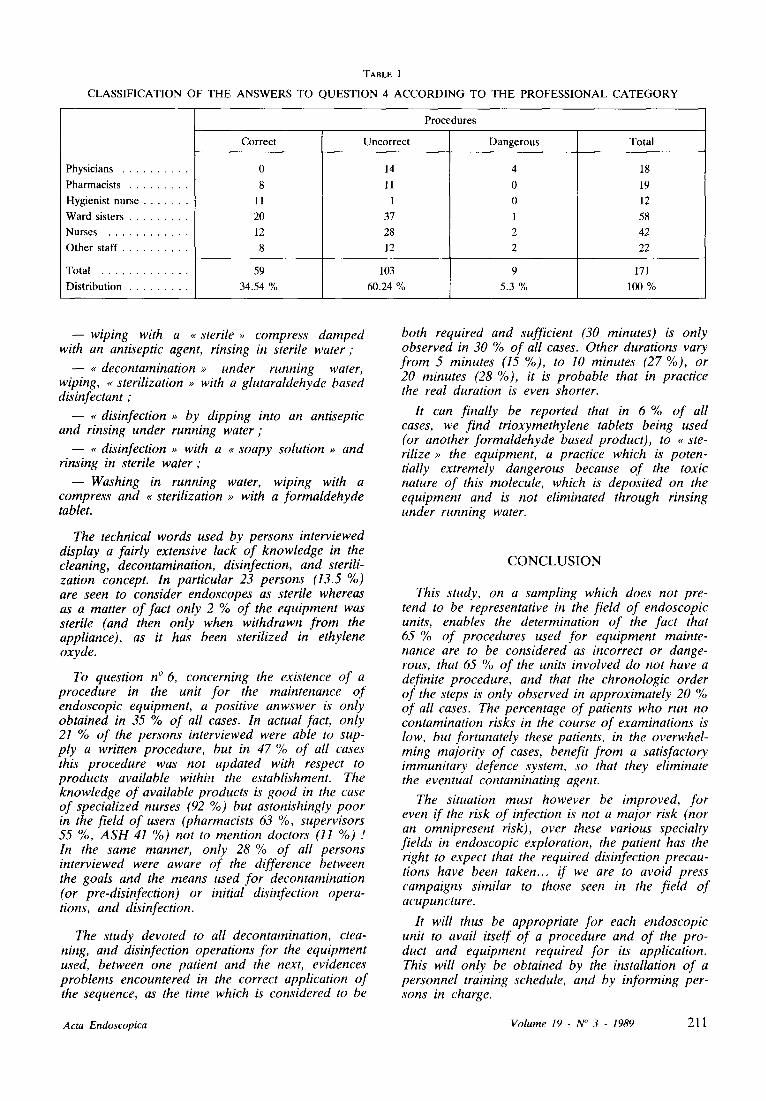
TABLE I
CLASSIFICATION OF THE ANSWERS TO QUESTION 4 ACCORDING TO THE PROFESSIONAL CATEGORY
Physicians
Pharmacists
Hygienist nurse
Ward sisters
Nurses
�9 Other staff . . . . . . . . . . .
Total
Distribution
Procedures
Correct Uncorrect Dangerous Total
0
8
11
20
12
8
14
11
1
37
28
12
18
19
12
58
42
22
59 lO3 9 171
34.54 % 60.24 % 5.3 % lOO %
- -wip ing with a ~ sterile ,, compress damped with an antiseptic agent, rinsing in sterile water ;
- - ~, decontamination ~ under running water, wiping, ~ sterilization ,~ with a glutaraldehyde based disinfectant ;
- - , , disinfection ~ by dipping into an antiseptic and rinsing under running water ;
- - ,~ disinfection ,~ with a ~ soapy solution ,~ and rinsing in sterile water ;
--Washing in running water, wiping with a compress and ~ sterilization ~, with a formaldehyde tablet.
The technical words used by persons interviewed display a fairly extensive lack of knowledge in the cleaning, decontamination, disinfection, and sterili- zation concept. In particular 23 persons (13.5 %) are seen to consider endoscopes as sterile whereas as a matter of fact only 2 % of the equipment was sterile (and then only when withdrawn from the appliance), as it has been sterilized in ethylene oxyde.
To question n ~ 6, concerning the existence of a procedure in the unit for the maintenance of endoscopic equipment, a positive anwswer is only obtained in 35 % of all cases. In actual fact, only 2 1 % of the persons interviewed were able to sup- ply a written procedure, but in 47 % of all cases this procedure was not updated with respect to products available within the establishment. The knowledge of available products is good in the case of specialized nurses (92 %) but astonishingly poor in the field of users (pharmacists 63 %, supervisors 55 %, ASH 41%) not to mention doctors (11%) .t In the same manner, only 28 % of all persons interviewed were aware of the difference between the goals and the means used for decontamination (or pre-disinfection) or initial disinfection opera- tions, and disinfection.
The study devoted to all decontamination, clea- ning, and disinfection operations for the equipment used, between one patient and the next, evidences problems encountered in the correct application of the sequence, as the time which is considered to be
both required and sufficient (30 minutes) is only observed in 30 % of all cases. Other durations vary from 5 minutes (15 %), to 10 minutes (27 %), or 20 minutes (28 %), it is probable that in practice the real duration is even shorter.
It can finally be reported that in 6 % of all cases, we find trioxymethylene tablets being used (or another formaldehyde based product), to ,, ste- rilize ,~ the equipment, a practice which is poten- tially extremely dangerous because of the toxic nature of this molecule, which is deposited on the equipment and is not eliminated through rinsing under running water.
C O N C L U S I O N
This study, on a sampling which does not pre- tend to be representative in the field of endoscopic units, enables the determination of the fact that 65 % of procedures used for equipment mainte- nance are to be considered as incorrect or dange- rous, that 65 % of the units involved do not have a definite procedure, and that the chronologic order of the steps is only observed in approximately 20 % of all cases. The percentage of patients who run no contamination risks in the course of examinations is low, but fortunately these patients, in the overwhel- ming majority of cases, benefit from a satisfactory immunitary defence system, so that they eliminate the eventual contaminating agent.
The situation must however be improved, for even if the risk of infection is not a major risk (nor an omnipresent risk), over these various specialty fields in endoscopic exploration, the patient has the right to expect that the required disinfection precau- tions have been taken.., if we are to avoid press campaigns similar to those seen in the field of acupuncture.
It will thus be appropriate for each endoscopic unit to avail itself of a procedure and of the pro- duct and equipment required for its application. This will only be obtained by the installation of a personnel training schedule, and by informing per- sons in charge.
Acta Endoscopica Volume 19 - N" 3 - 1989 21 1
A N N E X 1
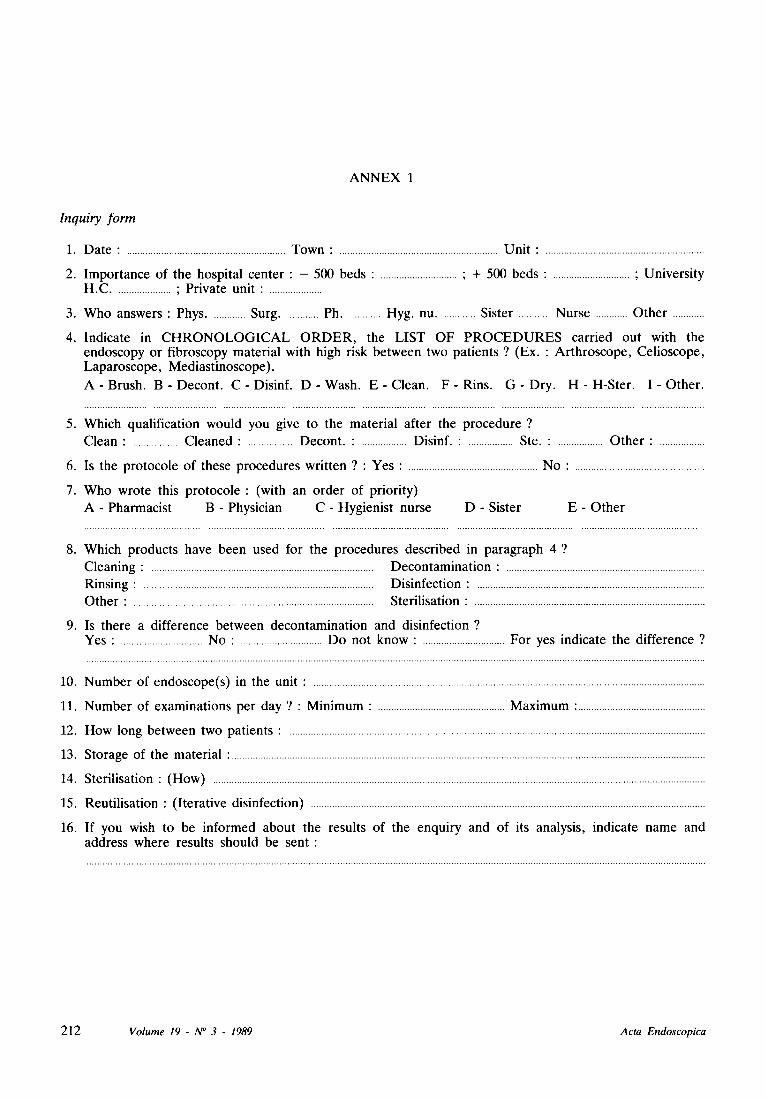
Inquiry form
1. D a t e : ............................................................ T o w n : ............................................................ U n i t : ............................................................
2. I m p o r t a n c e o f t h e h o s p i t a l c e n t e r : - 500 b e d s : ............................. ; + 500 b e d s : ............................. ; U n i v e r s i t y H . C ..................... ; P r i v a t e un i t : ....................
3. W h o a n s w e r s : Phys ............. Su rg ............. Ph ............. H y g . nu ............. S i s te r ............ N u r s e ............ O t h e r ............
4. I n d i c a t e in C H R O N O L O G I C A L O R D E R , t h e L I S T O F P R O C E D U R E S c a r r i e d o u t w i t h t h e e n d o s c o p y o r f i b r o s c o p y m a t e r i a l w i th h igh r isk b e t w e e n t w o p a t i e n t s ? (Ex . : A r t h r o s c o p e , C e l i o s c o p e , L a p a r o s c o p e , M e d i a s t i n o s c o p e ) .
A - B r u s h . B - D e c o n t . C - D i s i n f . D - W a s h . E - C l e a n . F - R i n s . G - D r y . H - H - S t e r . I - O t h e r .
5. W h i c h q u a l i f i c a t i o n w o u l d y o u g ive to t h e m a t e r i a l a f t e r t h e p r o c e d u r e ?
C l e a n : ................. C l e a n e d : ................. D e c o n t . : ................. D i s in f . : ................. S te . : ................. O t h e r : .................
6. Is t h e p r o t o c o l e o f t h e s e p r o c e d u r e s w r i t t e n ? : Y e s : ................................................. N o : .................................................
7. W h o w r o t e this p r o t o c o l e : (wi th an o r d e r o f p r i o r i t y )
A - P h a r m a c i s t B - Phys i c i an C - H y g i e n i s t n u r s e D - S i s te r E - O t h e r
8. W h i c h p r o d u c t s h a v e b e e n u s e d fo r t h e p r o c e d u r e s d e s c r i b e d in p a r a g r a p h 4 ?
C l e a n i n g : .................................................................................... D e c o n t a m i n a t i o n : ...........................................................................
R i n s i n g : ....................................................................................... D i s i n f e c t i o n : ......................................................................................
O t h e r : ........................................................................................... S t e r i l i s a t i on : .......................................................................................
9. Is t h e r e a d i f f e r e n c e b e t w e e n d e c o n t a m i n a t i o n a n d d i s i n f e c t i o n ? Y e s : ............................... N o : ............................... D o n o t k n o w : ............................... F o r yes i n d i c a t e t h e d i f f e r e n c e ?
10. N u m b e r o f e n d o s c o p e ( s ) in t h e un i t : ....................................................................................................................................................
11. N u m b e r o f e x a m i n a t i o n s p e r d a y ? : M i n i m u m : ................................................ M a x i m u m : ................................................
12. H o w l o n g b e t w e e n t w o p a t i e n t s : .............................................................................................................................................................
13. S t o r a g e o f t he m a t e r i a l : ...................................................................................................................................................................................
14. S t e r i l i s a t ion : ( H o w ) ..........................................................................................................................................................................................
15. R e u t i l i s a t i o n : ( I t e r a t i v e d i s i n f e c t i o n ) .....................................................................................................................................................
16. I f y o u wish to be i n f o r m e d a b o u t t h e resu l t s o f t h e e n q u i r y a n d o f its ana lys i s , i n d i c a t e n a m e a n d a d d r e s s w h e r e resu l t s s h o u l d be sen t :
212 V o l u m e 19 - N ~ 3 - 1989 A c t a E n d o s c o p i c a