Embed Size (px)
Citation preview
N o l e s l e c h n i q u e s I T e c h n i c a l r e p o r l s I l l i
Int6r t de la pHm6tr ie perendoscopique
Premiers r6sultats
F. VICARI, J. LAURENT, R. JEANPIERRE, B. WATRIN, A. JACQUIER Travail du G.R.P.D.N., 127, rue Saint-Dizier, 54000 Nancy
Service de M~decine H (Professeur J. Schmitt), H6pital Central, 29, avenue Mar~chal-de-Lattre-de-Tassigny, 54000 Nancy
Importance of perendoscopic pH metry First results
RF.SUMI~
Cette &ude pr61iminaire a pour but d'appr6cier l'apport de la pHm6trie perendoscopique comme exa- men de routine dans le cadre de la pathologic ~eso- gastro-duod6nale. Utilis~e au cours de toute endo- scopie haute, elle permet de d6tecter en particulier les hyper ou hypo-acidit6s gastriques totales ou foca-
lis6es. La pHm6trie permet en outre une surveillance de l'estomac soumis ?~ diverses th6rapeutiques m6di- cales ou chirurgicales. Une dizaine de patients ont 6t6 soumis tour ~t tour ~t une pHm6trie perendoscopique et ~t un tubage gastrique ~t la pentagastrine afin d'ap- pr6cier les corr61ations entre ces deux m6thodes.
S U M M A R Y
This prelinzinary study aims at estimating the contribution of perendoscopic pH metry as a routine examination in oeso-gastro-duodenal pathology. Used during any endoscopy of the upper GI tract, it allows a detection especially for the entire o/ /oealised gastric hyper or hypo-acidities. On an other hand. it
is also useful for the follow-up of the stomach sub- mitted to di[ferent medical or surgical therapies. About 10 patients underwent a perendoscopic pH merry and gastric intubation with pentagastrine in order to appreciate the correlations between both methods.
L'endoscopie permet dans le cadre de la pathologie ~esogastroduod6nale de r6aliser une 6tude morphologique, macroscopique et microscopique, de grande qualit& Mais Ie gastroent6rologue d6sire obtenir parall~lement
une &ude fonctionnelle de l'6tage digestif haut, portant en particulier sur la s6cr&ion acide gastrique. En clinique humaine, cette 6tude est r6alis6e habituetlement par le tubage gastrique avec stimulation h l'histamine ou
Tir~s ~t part : F. VICARI~ 127, rue Saint-Dizier, 54000 Nancy (France).
Mots-cl~s : pH endoscopie Key-words : pH endoscopy.
Acta Endoscopica Tome X - N o 3 - 1980 215
la pentagastrine. Cet examen, bien qu'ais6ment rdalisable, n'est pas tr6s confortable pour le patient et de ce fait, on peut difficilement proposer des tubages itdratifs pour suivre l'6volution d'une affection eesogastrique ou duoddnale.
L'dtude de la sdcrdtion gastrique acide a pu &re envisag6e depuis plus de vingt ans par des mesures pHmdtriques, grace ~ la raise en place d'dlectrodes ind6pendamment de tout repdrage endoscopique. Cette exploration pHmdtrique a 6t6 principalement utilis6e pour 6tudier le reflux gastro-eesophagien avec ou sans absorption d'acide chlorhydrique.
Nous rapportons les rdsultats d'une m6thode qui permet en un seul et m~me examen d'ap- pr6cier par l'endoscopie, la morphologie oeso- gastroduoddnale, et d'6tudier le pH, sous contrSle de la vue, dans les diff6rentes r6gions explor6es par l'endoscope.
M A T E R I E L E T M E T H O D E
L'6tude pHmdtrique est r6alis6e grfice / t u n pHm6tre Treier possddant une gamme de pH de 0 fi 12. I1 est muni de deux 61ectrodes : une macro-dlectrode de r6f6rence intra-buccale au chlorure d'argent et une micro-dlectrode perendoscopique de verre (diam~tre de 1,9 mm). Avant chaque mesure de pH, on d6termine la pente de l'61ectrode de verre. Toutes les mesures de pH sont rdalis6es sous contrSle de la vue, l'61ectrode ne g~nant en rien l'exploration endoscopique.
Cette 6tude pr61iminaire porte sur 90 pa- tients : 11 patients tdmoins ayant une gastro- scopie normale (histologie normale), 27 gas- trites, 20 ulc6res duoddnaux (dont 8 traitds mddicalement), 13 ulc~res gastriques (dont 9 traitds m6dicalement), 4 patients op6rds de l'estomac, 3 hernies hiatales, 2 reflux gastro- eesophagiens et enfin 10 patients ayant eu simultandment une pHm6trie et un tubage/~ la pentagastrine.
R E S U L T A T S
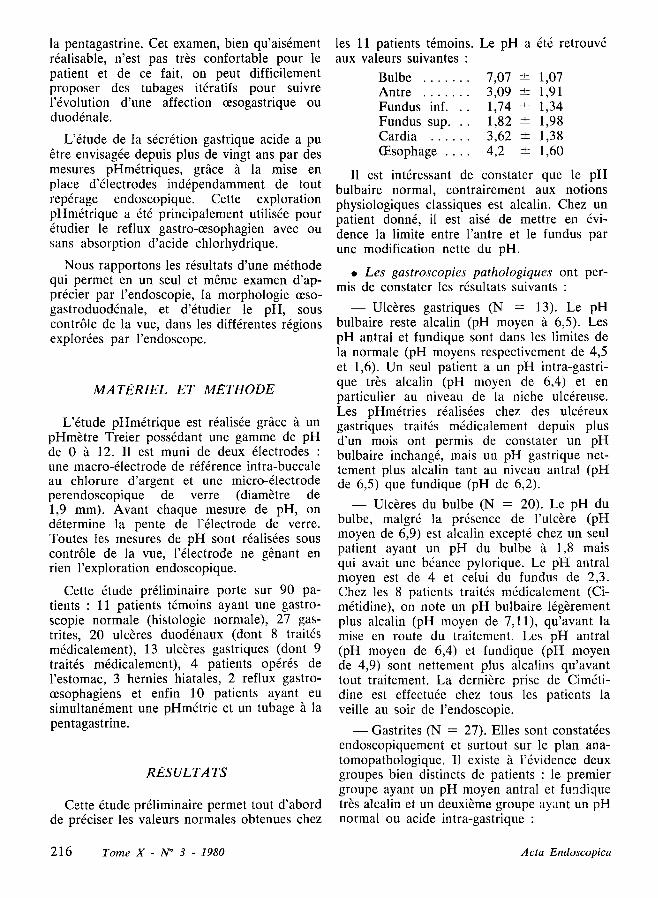
Cette 6tude pr61iminaire permet tout d'abord de pr6ciser les valeurs normales obtenues chez
les 11 patients t6moins. Le pH a 6t6 retrouv6 aux valeurs suivantes :
Bulbe . . . . . . . 7,07 • 1,07 Antre . . . . . . . 3,09 • 1,91 Fundus i n f . . . 1,74 • 1,34 Fundus s u p . . . 1,82 • 1,98 Cardia . . . . . . 3,62 • 1,38 (Esophage . . . . 4,2 • 1,60
II est intdressant de constater que le pH bulbaire normal, contrairement aux notions physiologiques classiques est alcalin. Chez un patient donn6, il est ais6 de mettre en 6vi- dence la limite entre l'antre et le fundus par une modification nette du pH.
�9 L e s gas troscopies pa tho log iques ont per- mis de constater les r6sultats suivants :
- - U l c 6 r e s gastriques (N = 13). Le pH bulbaire reste alcalin (pH moyen /t 6,5). Les pH antral et fundique sont dans les limites de la normale (pH moyens respectivement de 4,5 et 1,6). Un seul patient a un pH intra-gastri- que tr6s alcalin (pH moyen de 6,4) et en particulier au niveau de la niche ulc6reuse. Les pHm6tries r6alisdes chez des ulcdreux gastriques traitt~s m6dicalement depuis plus d'un mois ont permis de constater un pH bulbaire inchang6, mais un pH gastrique net- tement plus alcalin tant au niveau antral (pH de 6,5) que fundique (pH de 6,2).
- - Ulc6res du bulbe (N = 20). Le pH du bulbe, malgr6 la prdsence de l'ulc6re (pH moyen de 6,9) est alcalin except6 chez un seul patient ayant un pH du bulbe ~t 1,8 mais qui avait une b6ance pylorique. Le pH antral moyen est de 4 et celui du fundus de 2,3. Chez les 8 patients traitds mddicalement (Ci- mdtidine), on note un pH bulbaire ldg6rement plus alcalin (pH moyen de 7,11), qu'avant la raise en route du traitement. Les pH antral (pH moyen de 6,4) et fundique (pH moyen de 4,9) sont nettement plus alcalins qu'avant tout traitement. La derni6re prise de Cimdti- dine est effectu6e chez tous les patients la veille au soir de l'endoscopie.
- - Gastrites (N = 27). Elles sont constat6es endoscopiquement et surtout sur le plan ana- tomopathologique. II existe ~. l'6vidence deux groupes bien distincts de patients : le premier groupe ayant un pH moyen antral et funclique tr6s alcalin et un deuxi~me groupe ayant un pH normal ou acide intra-gastrique :
216 Tome X - N ~ 3 - 1980 Acta Endoscopica
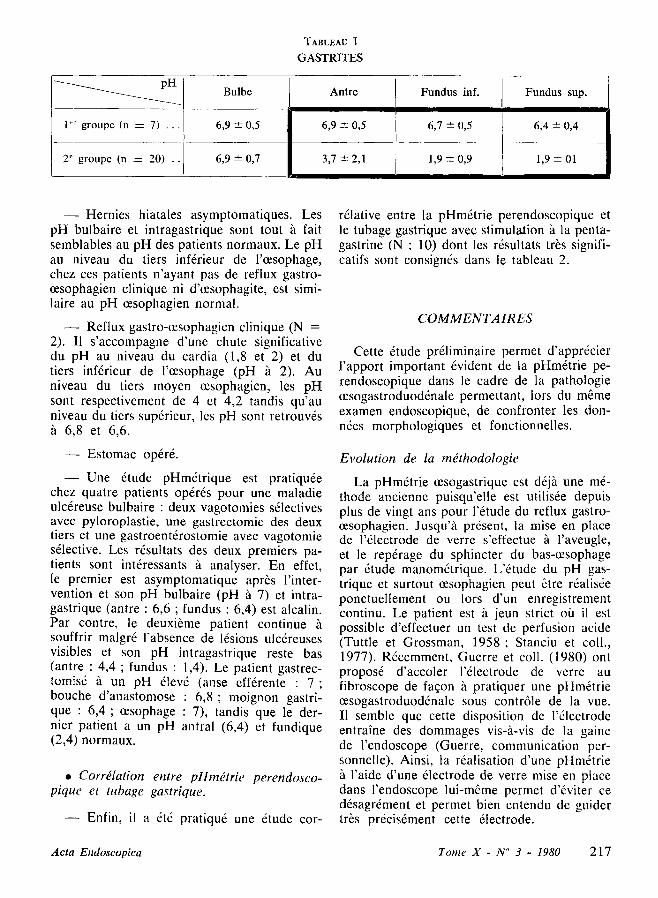
TABLEAU I
GASTRITES
p H
I"" groupe (n = 7) . . .
2" groupe (n = 20) ..
Bulbe
6,9 +- 0,5
6,9 • 0,7
Antre Fundus inf.
6,9 --+ 0,5 6,7 -+ 0,5
3,7 --- 2,1 1,9 --- 0,9
Fundus sup.
6,4 • 0,4
1,9 + 01
- - H e r n i e s hiatales asymptomatiques. Les pH bulbaire et intragastrique sont tout ~ fair semblables au pH des patients normaux. Le pH au niveau du tiers infdrieur de l'eesophage, chez ces patients n'ayant pas de reflux gastro- oesophagien clinique ni d'eesophagite, est simi- laire au pH eesophagien normal.
- - Reflux gastro-eesophagien clinique (N = 2). Il s 'accompagne d'une chute significative du pH au niveau du cardia (1,8 et 2) et du tiers inf6rieur de l'eesophage (pH ~t 2). Au niveau du tiers moyen eesophagien, les pH sont respectivement de 4 et 4,2 tandis qu'au niveau du tiers sup6rieur, les pH sont retrouv6s fi 6,8 et 6,6.
- - Estomac op6rd.
- - U n e 6tude pHm&rique est pratiqu6e chez quatre patients op6r6s pour une maladie ulc6reuse bulbaire : deux vagotomies s61ectives avec pyloroplastie, une gastrectomie des deux tiers et une gastroent6rostomie avec vagotomie s61ective. Les r6sultats des deux premiers pa- tients sont int6ressants 5' analyser. En effet, le premier est asymptomatique apr6s l'inter- vention et son pH bulbaire (pH 5' 7) et intra- gastrique (antre : 6,6 ; fundus : 6,4) est alcalin. Par contre, le deuxi6me patient continue 5' souffrir malgr6 l'absence de 16sions ulc6reuses visibles et son pH intragastrique reste bas (antre : 4,4 ; fundus : 1,4). Le patient gastrec- totals6 5. un pH dlev6 (anse eff6rente : 7 ; bouche d'anastomose : 6 ,8 ; moignon gastri- que : 6 ,4 ; cesophage : 7), tandis que le der- nier patient a un pH antral (6,4) et fundique (2,4) normaux.
�9 CorrOlation entre pHmdtr ie perendosco- pique et tubage gastrique.
- - Enfin, il a 6t6 pratiqu6 une 6tude cor-
r~lative entre la pHmdtrie perendoscopique et le tubage gastrique avec stimulation 5_ la penta- gastrine (N : 10) dont les r6sultats tr~s signifi- catifs sont consign6s dans le tableau 2.
C O M M E N T A 1R ES
Cette 6tude pr61iminaire permet d'appr6cier l 'apport important 6vident de la pHm6trie pe- rendoscopique dans le cadre de la pathologie oesogastroduod6nale permettant, lors du m~me examen endoscopique, de confronter les don- n6es morphologiques et fonctionnelles.
Evolut ion de la mdthodologie
La pHm6trie eesogastrique est d6j~. une m6- thode ancienne puisqu'elle est utilisfie depuis plus de vingt ans pour l'6tude du reflux gastro- eesophagien. Jusqu'~. pr6sent, la mise en place de l'61ectrode de verre s'effectue 5' l'aveugle, et le rep6rage du sphincter du bas-cesophage par 6tude manom6trique. L'dtude du pH gas- trique et surtout oesophagien peut 6tre r6alis6e ponctuellement ou lors d'un enregistrement continu. Le patient est ~. jeun strict ofa il est possible d'effectuer un test de perfusion acide (Tuttle et Grossman, 1958; Stanciu et coll., 1977). R6cemment, Guerre et coll. (1980) ont propos6 d'accoler l'61ectrode de verre au fibroscope de faqon 5. pratiquer une pHm6trie eesogastroduod6nale sous contr61e de la vue. I1 semble que cette disposition de l'61ectrode entraine des dommages vis-~.-vis de la gaine de l 'endoscope (Guerre, communication per- sonnelle). Ainsi, la r6alisation d'une pHm6trie 5. I'aide d'une 61ectrode de verre mise en place dans l'endoscope lui-m6me permet d'6viter ce d6sagr6ment et permet bien entendu de guider tr6s pr6cis6ment cette 61ectrode.
Acta Endoscopica Tome X - N ~ 3 - 1980 217
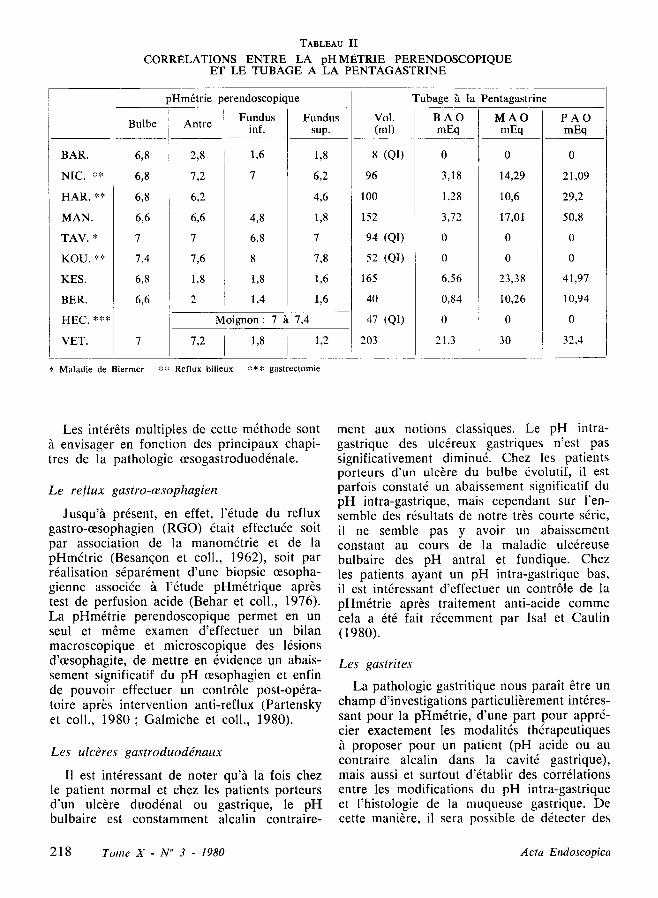
TABLEAU II CORRI~LATIONS ENTRE LA pHMi~,TRIE PERENDOSCOPIQUE
ET LE TUBAGE A LA PENTAGASTRINE
Bulbe
BAR. 6,8
NIC. ** 6,8
HAR. ** 6,8
MAN. 6,6
TAV. * 7
KOU. * * 7,4
KES. 6,8
BER. 6,6
HEC. ***
VET. 7
~Hm6trie perendoscopique
Antre
2,8
7,2
6,2
6,6
7
7,6
1,8
Fundus Fundus inf. sup.
1,6 1,8
7 6,2
4,6
4,8 1,8
6,8 7
8 7,8
1,8 1,6
1,4 1,6
Moignon: 7 ~t 7,4
7,2 1,8 1,2
Tubage ~t la Pentagastrine
Vol. BAO M A O P A O (ml) mEq mEq mEq
8 (QI)
96
100
152
94 (QI)
52 (QI)
165
4O
47 (QI)
203
0
3,18
1,28
3,72
0
0
6,56
0,84
0
21,3
0
14,29
10,6
17,01
0
0
23,38
10,26
0
30
0
21,09
29,2
50,8
0
0
41,97
10,94
0
32,4
* Maladie de Biermer ** Reflux bilieux *** gastrectomie
Les int6r6ts multiples de cette m6thode sont ft. envisager en fonction des principaux chapi- tres de la pathologie 0esogastroduoddnale.
L e r e f l u x g a s t r o - c e s o p h a g i e n
Jusqu'h pr6sent, en effet, l'6tude du reflux gastromesophagien (RGO) 6tait effectu6e soit par association de la manom6trie et de la pHm6trie (Besanqon et coll., 1962), soit par r6alisation s6par6ment d'une biopsie cesopha- gienne associ6e ~, l '6tude pHm6trique apr6s test de perfusion acide (Behar et coll., 1976). La pHm&rie perendoscopique permet en un seul et m~me examen d'effectuer un bilan macroscopique et microscopique des 16sions d'oesophagite, de mettre en 6vidence un abais- sement significatif du pH eesophagien et enfin de pouvoir effectuer un contr61e post-op6ra- toire apr6s intervention anti-reflux (Partensky et coll., 1980; Galmiche et coll., 1980).
L e s ulcOres g a s t r o d u o d ~ n a u x
II est int6ressant de noter qu'h la fois chez le patient normal et chez les patients porteurs d'un ulc6re duod6nal ou gastrique, le pH bulbaire est constamment alcalin contraire-
ment aux notions classiques. Le pH intra- gastrique des ulc6reux gastriques n'est pas significativement diminu& Chez les patients porteurs d'un ulc6re du bulbe 6volutif, il est parfois constat6 un abaissement significatif du pH intra-gastrique, mais cependant sur l 'en- semble des r6sultats de notre tr~s courte sdrie, il ne semble pas y avoir un abaissement constant au cours de la maladie ulcdreuse bulbaire des pH antral et fundique. Chez les patients ayant un pH intra-gastrique bas, il est int6ressant d'effectuer un contr61e de la pHm6trie apr6s traitement anti-acide comme cela a 6t6 fait r6cemment par Isal et Caulin (1980).
L e s gas t r i t e s
La pathologie gastritique nous para~t 6tre un champ d'investigations particuli6rement int6res- sant pour la pHm&rie, d'une part pour appr6- cier exactement les modalit6s th6rapeutiques
proposer pour un patient (pH acide ou au contraire alcalin dans la cavit6 gastrique), mais aussi et surtout d'6tablir des corr61ations entre les modifications du pH intra-gastrique et l'histologie de la muqueuse gastrique. De cette mani~re, il sera possible de d6tecter des
218 Tome X - N ~ 3 - 1980 Acta Endoscopica
gastrites atrophiques avec pH alcalin et des zones de m6taplasies intestinales, ces deux 16sions constituant des terrains de pr6dilection pour l'6closion du cancer gastrique. Nous avons pu d6tecter de cette mani~re chez un patient une zone tr6s nette d'alcalinit6 antrale correspondant h une zone de m6taplasie intes- tinale au sein de laquelle il a 6t6 possible de mettre en 6vidence un n6oplasme gastrique in situ.
Ainsi, la pHm6trie perendoscopique dont nous ne pr6sentons ici qu'une 6tude pr61imi- naire nous parait &re un examen de r6alisation
facile et fiable permettant if&re effectu6 de fa~on it6rative. L'6tude simultan6e des aspects morphologiques et fonctionnels ~t l'6tage di- gestif haut est ainsi rendue possible par un examen non agressif et confortable pour le patient. La pHm6trie permet en outre une surveillance des diverses th6rapeutiques m6di- cales et chirurgicales vis-?t-vis du reflux gastro- eesophagien, de la maladie ulc~reuse gastro- duod6nale et enfin des gastrites. Enfin, nous pensons que la pHmdtrie pourra apporter des renseignements tr~s utiles dans la d6tection des Stats pr&n6oplasiques gastriques que sont la gastrite atrophique et la m6taplasie intestinale.
BIBLIOGRAPHIE
BEHAR l., BIANCANI P., SHEAHAN D.G. - - Eva- luation of esophageal tests in the diagnosis of reflux esophagitis. Gasetroenterology, 1976, 71, 9-15.
BENZ L.J., HOOTKIN L.A., MARGULIES S., D O N N E R M.W., C A U T H O R N E R.T., HENDRIX T.R. - - A comparison of clinical measurements of gastroesopageal reflux. Gastroenterology, 1972, 62, 1-5.
BESANGON F., BAUJAT J.P., DEBRAY Ch. - - Le reflux gastro-eesophagien : Etude pHgraphique et 61ectromanographique. Sem. Hop. Paris, 1962, 26, 1569-1576.
G A L M I C H E J.P., GUILLARD J.F., DENIS P., TESTART J. ,COLIN R. - - Etude du pH cesopha- gien en p~riode post-prandiale chez le sujet normal et au cours du syndrome de reflux gastro-oesopha- gien. Int6r& d'un score de reflux acide. Gastro- enterol. Clin. Biol., 1980, 4, 1 bis, 162 A.
G U E R R E J., G A U D R I C M., BARS L., NEPVEUX P. - - Mesure du pH oeso-gastro-duod~nal pendant
l'endoscopie. Technique. Premiers r&ultats. Gastro- enterol. Clin. Biol., 1980, 4, 1 bis, 121 A.
ISAL J.P., CAULIN C. - - Effet sur le pH gastrique de l 'homme de diff6rents anti-acides et de la Cim&idine (Etude radiot616m&rique de 140 cas). Gastroenterol. Clin. Biol., 1980, 4, 1 bis, 155 A.
KAYE M.D. - - Postprandial gastro-oesophageal re- flux in healthy people. Gut, 1977, 18, 709-712.
PARTENSKY C., SAUBIER E.C., LEVEQUE A.M., BERETVAS G., MINAISE Y. - - Apport de la pHm&rie 0esophagienne dans la chirurgie du reflux gastro-0esophagien. Gastroenterol. Clin. Biol., 1980, 4, 1 bis, 161 A.
STANCIU C., H O A R E R.C., BENNETT J.R. - - Correlation between manometric and pH tests for gastro-oesophageal reflux. Gut, 1977, 18, 536-540.
TUTTLE S.G., GROSSMAN M.I. - - Detection of gastro-esophageal reflux by simultaneous measure- ment of intraluminal pressure and pH. Proceedings of the Society for Experimental biology and Medi- cine, 1958, 98, 225-227.
In oeso-gastro-duodenal pathology, endo- scopy allows the realisation of a morphological macroscopic and microscopic study of high quality. But the gastroenterologist needs to obtain in parallel a functional study of the upper GI tract, especially oriented on the gastric acid secretion. In human clinic, this study is usually realised by gastric intubation with histamine or pentagastrine stimulation. This investigation although easily performed, is not very comfortable for the patient and for that reason it is difficult to propose iterative intubations to follow the evolution of an oeso- gastric or duodenal affection.
The study o] the gastric acid secretion has been realised for more than 20 years through pH metric measurements thank to the setting of electrodes independently of any endoscopic indications. This pH metric exploration was mainly used to study the gastro-oesophageal reflux with or without any absorption of chlor- hydric acid.
We report the results of a method allowing in the only one and same examination to appre- ciate endoscopically the oeso-gastro-duodenaI morphology and to study the pH, under view control in the different areas explored by the endoscope.
Acta Endoscopica Tome X - N ~ 3 - 1980 219
M A T E R I A L A N D M E T H O D S
The pH metric study is realised through a Treier pH metre with a pH range from 0 to 12. It is supplied with 2 electrodes : a macro electrode with intra buccal reference made of chlorure of silver and a perendoscopic micro electrode made of glass (diameter : 1.9 mm). Before each pH measurements, the inclination of the glass electrode is determined. All the pH measurements are realised under view control, the electrode does not prevent in any way the endoscopic exploration.
Thhr preliminary study is carried out on 90 patients : 11 patients (check sample) with normal gastroscopy (normal histology), 27 gas- tritis, 20 duodenal ulcers (among them 8 medi- cally treated), 13 gastric ulcers (among them 9 medically treated), 4 patients having under- gone an operation of the stomach, 3 hiatal hernia, 2 gastro-oesophageal reflux and finally 10 patients having undergone simultaneously a pH metry and a pentagastrine intubation.
R E S U L T S
This preliminary study first of all, precises the normal values obtained in the 11 patients choosen as check sample. The pH values were the following :
Bulb . . . . . . . . . 7.07 • 1.07
Antrum . . . . . . . 3.09 ++- 1.91
Inf. Jundus . . . . 1.74 +- 1.34
Sup. Jundus . . . . 1.82 +- 1.98
Cardia . . . . . . . . 3.62 • 1.38
Oesophagus . . . . 4.20 +- 1.60
It is interesting to notice that the normal
bulbar pH, contrary to the classical physio- logical notions, is alcaline. On a determined patient it is easy to show the limits between the antrum and the fundus because of the pH modification.
�9 T h e p a t h o l o g i c g a s t r o s c o p i e s could lead to the following results :
- - Gastric ulcers (N = 13). The bulbar pH remains alcaline (average pH : 6.5). The antral and fundic pH are in the limits of normality (average pH respectively of 4.5 and 1.6). Only one patient has a lull alcaline intra-gastric pH (average pH : 6.4) and particularly at the level of the ulcerous niche. The pH metries realised on gastric ulcerous patients medically treated for more than 1 month could show an in- change bulbar pH, but a gastric pH being evidently more alcaline, as well at the antral level (pH : 6.5) as at the fundic level (pH : 6.2).
- - Bulb ulcers (N = 20). The bulb pH inspite of the presence of the ulcer (average pH : 6.9) is alcaline except in an only patient having a bulb pH of 1.8 but who suffered from a pyloric open bite. The average antral pH is of 4 and the Jundic pH of 2.3. In 8 pa- tients medically treated (cimetidine), the bulbar pH is slightly more alcaline (average pH of 7.11) than before the setting of the treatment. The antral (average pH : 6.4) and fundic pH (average pH : 4.9) are far more alcaline than before any treatment. The last take of cime- tidine occurs in all patients on the evening before the endoscopy.
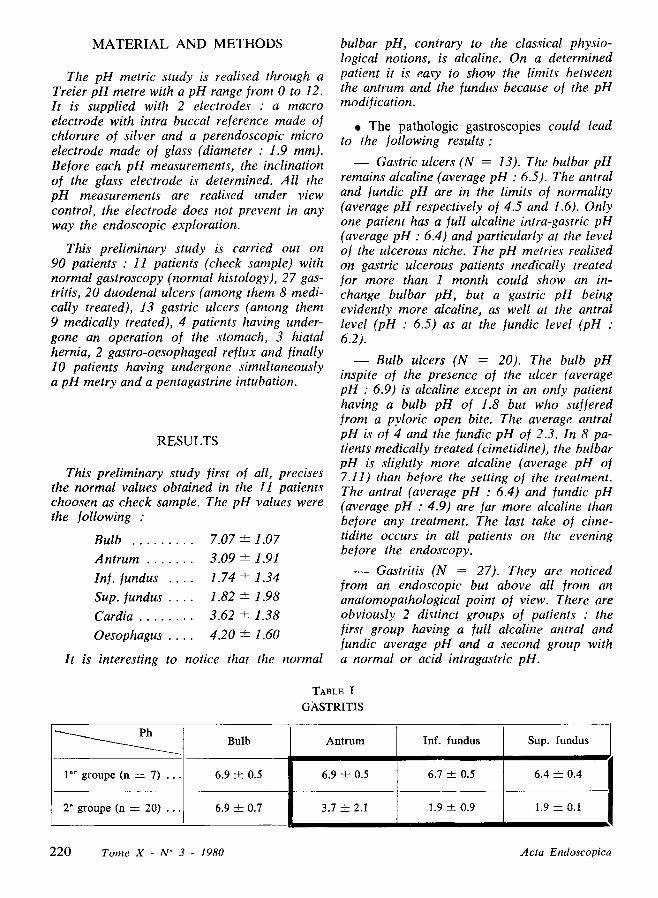
- - Gastritis (N = 27). They are noticed from an endoscopic but above all from an anatomopathological point of view. There are obviously 2 distinct groups of patients : the first group having a full alcaline antral and fundic average pH and a second group with a normal or acid intragastric pH.
Ph
1 er groupe (n = 7) . .
2 e groupe (n ---- 20) . . 6.9 ___ 0.7
Bulb
6.9 4- 0.5
3.7 __+ 2.1
A n t r u m
6.9 -4- 0.5
TABLE I
G A S T R I T I S
Inf. fundus
6.7 ___ 0.5
1.9 -+- 0.9
Sup. fundus
6.4 ___ 0.4
1.9 • 0.I
2 2 0 Tome X - N" 3 - 1980 Acta Endoscopica
- - Asymptomatic hiatal hernia. The bulbar and intragastric pH are the same as the one of normal patients. The pH at the level of the inferior 1/3 of the oesophagus, in these pa- tients with no clinical gastro-oesophageal re- flux or oesophagitis, is similar to the normal oesophageal pH.
- - Clinical gastro-oesophageal reflux (N = 2). It is related to a significant fall oJ the pH at the level of the cardia (1.8 and 2) and of the inferior 1/3 of the oesophagus (pH : 2). At the level of the intermediate 1/3 of the oesopha- gus, the pH are respectively of 4 and 4.2 whereas at the level oJ the cervical oesophagus, the pH values are o[ 6.8 and 6.6.
- - Operated stomach. A pH metric study is carried out, on 4 patients having undergone an operation for a bulbar ulcerous disease : 2 se- lective vagotomies with pyloroplasty, a gastrec- tomy of the 2 thirds and a gastroenterostomy with a selective vagotomy. It is interesting to
analyse the results of the 2 ]irst patients. As a matter of fact, the first one is asymptomatic after the operation and his bulbar (pH : 7) and intragastric pH (antrum : 6.6, fundus : 6.4) is alcaline. But on another hand, the second patient keeps on su]fering inspite o] the missing o] visible ulcerous lesions and his intragastric pH remains low (antrum : 4.4, ]un- dus : 1.4). The patient having undergone a gastrectomy has a high pH (efferent ansa : 7, anastomosis : 6.8, gastric stump : 6.4, oeso- phagus : 7), whereas the last patient has a normal antral (6.4) and ]undic (2.4) pH.
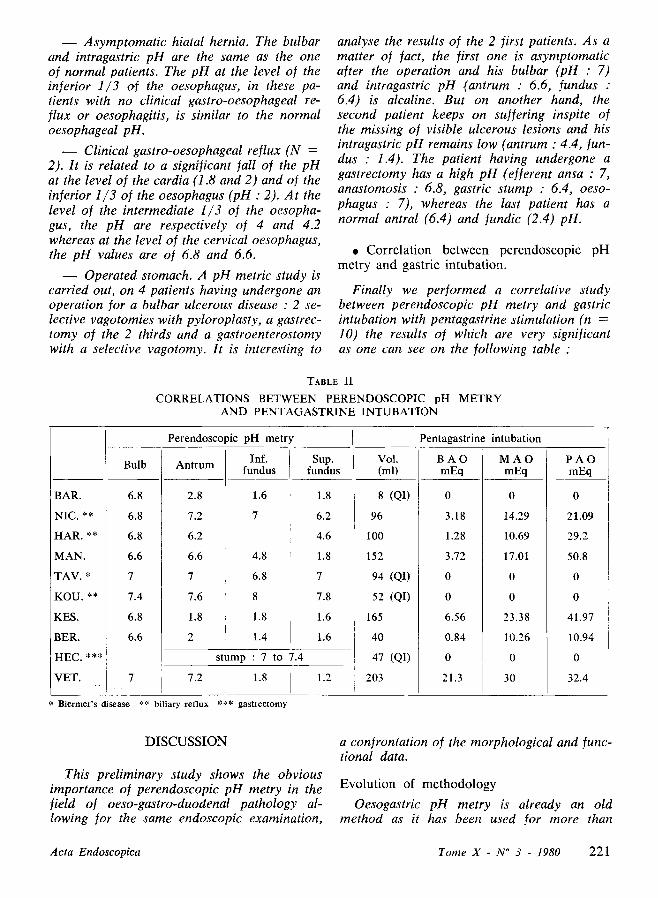
�9 C o r r e l a t i o n b e t w e e n p e r e n d o s c o p i c p H m e t r y a n d g a s t r i c i n t u b a t i o n .
Finally we performed a correlative study between perendoscopic pH metry and gastric intubation with pentagastrine stimulation (n = 10) the results of which are very significant as one can see on the following table :
TABLE II
CORRELATIONS BETWEEN PERENDOSCOPIC pH METRY A N D P E N T A G A S T R I N E I N T U B A T I O N
BAR.
NIC. **
HAR. **
MAN.
TAV. *
KOU. **
KES.
BER.
HEC. ***
VET.
Perendoscopic pH metry Pentagastrine intubation
Bulb Sup. Vol. P A O fundus (ml) mEq
6.8
6.8
6.8
6.6
7
7.4
6.8
6.6
7
Inf. Ant rum fundus
2.8 1.6
7.2 7
6.2
6.6 4.8
7 6.8
7.6 8
1.8 1.8
2 1.4
stump : 7 to 7.4
1.8
6.2
4.6
1.8
7
7.8
1.6
1.6
7.2 1.8 1.2
8 (QI)
96
I00
152
94 (QI)
52 (QI)
165
40
47 (QI)
203
B A O M A O mEq mEq
0 0
3.18 14.29
1.28 10.69
3.72 17.01
0 0
0 0
6.56 23.38
0.84 10.26
0 0
21.3 30
0
21.09
29.2
50.8
0
0
41.97
10.94
0
32.4
Biermer's disease ~.~* biliary reflux *** gastreetomy
D I S C U S S I O N
This preliminary study shows the obvious importance oJ perendoscopic pH metry in the field of oeso-gastro-duodenal pathology al- lowing 1or the same endoscopic examination,
a con]rontation of the morphological and Junc- tional data.
E v o l u t i o n of m e t h o d o l o g y
Oesogastric pH metry is already an old method as it has been used for more than
Acta Endoscopica Tome X - N ~ 3 - 1980 221

20 years ]or the study of the gastro-oeso- phageal reflux. Up to now, the setting of the glass electrode has been performed blindly and the landmarking of the low oesophagus sphincter by a manometric study. The study of gastric and above all of oesophageal pH may be realised punctually or during a conti- nuous recording. The patient observes a strict fast which is required to perform an acid perfusion test (Tuttle and Grossman, 1958 ; Stanciu and coll., 1977). Recently, Guerre and coll. (1980) proposed to supply the fibroscope with a glass electrode in order to perform an oeso-gastro-duodenal pH metry under view control. This setting of the electrode damages the sheath of the fiberscope (Guerre, personal report). Thus, pH metry performed with a glass electrode in the fiberscope itself prevents this drawback and gives a good precision in the guiding of this electrode. The numerous ad- vantages of this method are to be considered according to the main parts of oeso-gastro- duodenal pathology.
Gastro-oesophageal reflux
In fact, up to now, the study of gastro- oeso- phageal reflux (G.O.R.) has been performed either by the association of manometry and pH metry (Besanfon and coll., 1962) or by the realisation of an oesophageal biopsy com- bined with the pH metric study after acid perfusion test (Behar and coll., 1976). Peren- doscopic pH metry allows in the only one and same investigation to carry out a macroscopic and microscopic check up of the oesophageal lesions to show a significant fall in oesophageal pH and finally to have a post-surgical control after the anti-reflux intervention (Partensky and coll., 1980 ; Galmiche and coll., 1980).
Gastro-duodenal ulcers
It is interesting to notice that either on normal patients or on patients carrying a duo- denal or gastric ulcer, bulbar pH is constantly alcaline, contrarily to the classical notions,
gastric pH in gastric ulcerous patients is not significantly reduced.
On patients carrying an evolutive bulbar ulcer, a significant Jail of the intra-gastric pH can be noticed, but nevertheless, considering all the results of our very short series, there does not seem to be a constant fall of antral and fundic pH during the bulbar ulcerous disease. In patients with a long intragastric pH, it is interesting to perform a pH metric control after an anti-acid treatment as it was recently done by Isal and Caulin (1980).
Gastritis
Gastritic pathology seems to be a particu- larly interesting investigation field for pH merry, on one hand, to appreciate exactly the therapeutic modalities for the patient (acid pH or on the contrary, alcaline pH in the gastric cavity) but also and above all to establish correlations between the intragastric pH modi- fications and the histology of the gastric mu- cosa. So it will be possible to detect atrophic gastritis with alcaline pH and metaplasic intes- tinal areas, these 2 lesions being Javourable to develop gastric cancer. We could thus detect in a patient an area with obvious antral alcalinity corresponding to a metaplastic intestinal area inside which an in-situ gastric neoplasm was discovered.
Thus perendoscopic pH merry, here only presented through a preliminary study, seems to be an easy and liable examination which can be performed in an iterative way. The si- multaneous study of the morphological and functional aspects of the upper GI tract is now possible with a non-agressive and comfortable examination for the patient, pH metry on an other hand allows a control of the different medical and surgical therapies concerning gastro-oesophageal reflux, gastro-duodenal ul- cerous disease and finally gastritis.
Finally, we think that pH merry will be able to bring useful informations in the detection of gastric pre-neoplasic stages such as atrophic gastritis or intestinal metaplasia.
222 Tome X - N ~ 3 - 1980 Acta Endoscopica