Embed Size (px)
Citation preview
T
S
Ac(
A
a
Pb
1
RA
1
Itgfcit
f
0d
ransactions of the Royal Society of Tropical Medicine and Hygiene (2009) 103, 1288—1290
avai lab le at www.sc iencedi rec t .com
journa l homepage: ht tp : / /www.e lsev ier .com/ locate / t rs tmh
HORT COMMUNICATION
bsence of an impact of resistance to chloroquine ononsultations for malaria in Niakhar, Senegal1992—2004)
. Muniera,b,∗, A. Diallob, J.P. Chippauxa
Institut de recherche pour le développement (IRD), UR010 ‘Santé de la mère et de l’enfant en milieu tropical’, Faculté deharmacie, Université Paris Descartes, 4 Ave. de l’Observatoire, 75006 Paris, FranceInstitut de recherche pour le développement (IRD), US009 ‘Suivi démographique, épidémiologique et environnemental’, BP386 Dakar, Senegal
eceived 3 February 2009; received in revised form 17 March 2009; accepted 17 March 2009vailable online 25 April 2009
KEYWORDSMalaria;Antimalarial drugs;
Summary We retrospectively assessed the impact of chloroquine (CQ) resistance in the ruralregion of Niakhar, Senegal, where resistance to CQ emerged in 1992, from increases in con-sultations and returns of patients to the health centre following antimalarial treatment. No
Chloroquine;Drug resistance;Healthcare facilities;Senegal
significant differences were observed between 1992, when chemoresistance appeared, and2004, when first-line treatment of malaria changed, except in the private centre where prac-tices and follow-up were distinct. In this zone of Senegal, resistance to CQ does not appear tohave a high impact on malaria morbidity in health centres.
opica
tiwiT
© 2009 Royal Society of Trreserved.
. Introduction
n the rural area of Niakhar, West Senegal, resistanceo chloroquine (CQ) emerged in 1992 and increasedradually.1,2 However, CQ remained the first-line treatmentor malaria until 2003, when it was replaced by the asso-
iation amodiaquine + sulfadoxine/pyrimethamine. Quininenjections were mainly used for severe malaria. No resis-ance to quinine has been observed.3∗ Corresponding author. Tel.: +33 1 5373 1506;ax: +33 1 5373 9617.
E-mail address: munier [email protected] (A. Munier).
f
2
Tslit
035-9203/$ — see front matter © 2009 Royal Society of Tropical Medicinoi:10.1016/j.trstmh.2009.03.017
l Medicine and Hygiene. Published by Elsevier Ltd. All rights
On the occasion of a study on the consequences of resis-ance to CQ in the Niakhar area, we evaluated increasesn consultations for malaria and returns of patients treatedith CQ in comparison with those treated with quinine as
ndicators of a possible decrease in the efficacy of CQ.he evolution of both indicators was studied retrospectivelyrom 1992 to 2004.
. Patients and methods
he study was conducted in the rural zone of Niakhar, 130 kmoutheast of Dakar, Senegal, a demographic surveillance siteocated in the Sahelo-Sudanese region of Fatick4 and cover-ng a population of 30 000 inhabitants on average from 1992o 2004.
e and Hygiene. Published by Elsevier Ltd. All rights reserved.
egal 1289
etur
nsof
pati
ents
toth
edi
spen
sary
betw
een
Day
1an
dD
ay28
acco
rdin
gto
the
pres
crib
edan
tim
alar
iald
rug
and
the
heal
thca
refa
cilit
y,19
92—
2004
,N
iakh
arst
udy
al vate
cent
re(D
iohi
ne)
Publ
icce
ntre
s(T
ouca
ran
dN
gayo
khem
)
sum
ptiv
eca
ses+
CQa
Retu
rnaf
ter
CQ[n
(%)]
Pres
umpt
ive
case
s+Q
(n)b
Retu
rnaf
ter
Q[n
(%)]
Pres
umpt
ive
case
s+CQ
(n)a
Retu
rnaf
ter
CQ[n
(%)]
Pres
umpt
ive
case
s+Q
(n)b
Retu
rnaf
ter
Q[n
(%)]
12c
3(1
.4)
139
14(1
0.1)
140
0(0
.0)
241
(4.2
)20
25(3
.0)
226
13(5
.8)
211
6(2
.8)
100
4(4
.0)
4314
(1.7
)16
13
(1.9
)17
10
(0.0
)39
0(0
.0)
0922
(2.4
)47
1(2
.1)
369
8(2
.2)
875
(5.7
)43
12(1
.9)
103
4(3
.9)
835
18(2
.2)
212
6(2
.8)
4913
(2.0
)72
1(1
.4)
455
4(0
.9)
931
(1.1
)67
48(5
.0)
458
72(1
5.7)
798
20(2
.5)
193
4(2
.1)
0659
(8.4
)57
292
(16.
1)59
215
(2.5
)15
52
(1.3
)58
34(7
.4)
481
73(1
5.2)
794
12(1
.5)
221
3(1
.4)
8866
(11.
2)69
213
3(1
9.2)
801
17(2
.1)
192
3(1
.6)
2727
(6.3
)71
283
(11.
7)71
413
(1.8
)19
84
(2.0
)75
6(3
.4)
556
70(1
2.6)
483
8(1
.7)
814
12(1
.5)
491
(2.0
)21
75
(2.3
)4
0(0
.0)
1409
13(0
.9)
4633
0(4
.4)
4436
564
(12.
7)63
6712
1(1
.9)
3737
58(1
.6)
e;Q
:qu
inin
e.
ith
acl
inic
alm
alar
iadi
agno
sis
and
pres
crip
tion
ofCQ
alon
e.it
ha
clin
ical
mal
aria
diag
nosi
san
dpr
escr
ipti
onof
Qal
one.
ding
Dio
hine
disp
ensa
ryw
ere
inco
mpl
ete
in19
92(a
vaila
ble
July
—D
ecem
ber
only
).
Absence of clinical impact of resistance to chloroquine, Sen
Three healthcare facilities located in the villages of Dio-hine (private catholic dispensary), Toucar and Ngayokhem(public health centres) carry out primary healthcare ser-vices. Health records from the period 1992—2004 werecollected retrospectively, including the date of consultation,name, sex and age of patients, clinical signs, diagno-sis and treatment prescribed by the nurse. A total ofapproximately 8500 consultations per year were performedin these centres. Malaria diagnosis was based on clini-cal symptoms only and was made by the nurse in chargeof the consultations, as no laboratory facility was avail-able.
Returns of patients were identified after selection byname, sex, village of residence and age. The rate of returnswas defined as patients with a clinical diagnosis of malariaat the first consultation and treated with antimalarials whoreturned to the dispensary between Day 1 and Day 28 withpersistent signs of disease. The evolution of the rate ofreturns from 1992 to 2004 was observed, and the number ofpatients treated with CQ was compared with those treatedwith quinine at the first visit.
Patients receiving a simultaneous prescription of qui-nine as ‘attack treatment’ and CQ as relay treatment aswell as those receiving other antimalarials were excluded.Statistical analysis was performed using Stata 8.0 software(StataCorp LP, College Station, TX, USA). Proportions werecompared using Pearson’s �2 test. Statistical significance wasset to P = 0.05.
3. Results
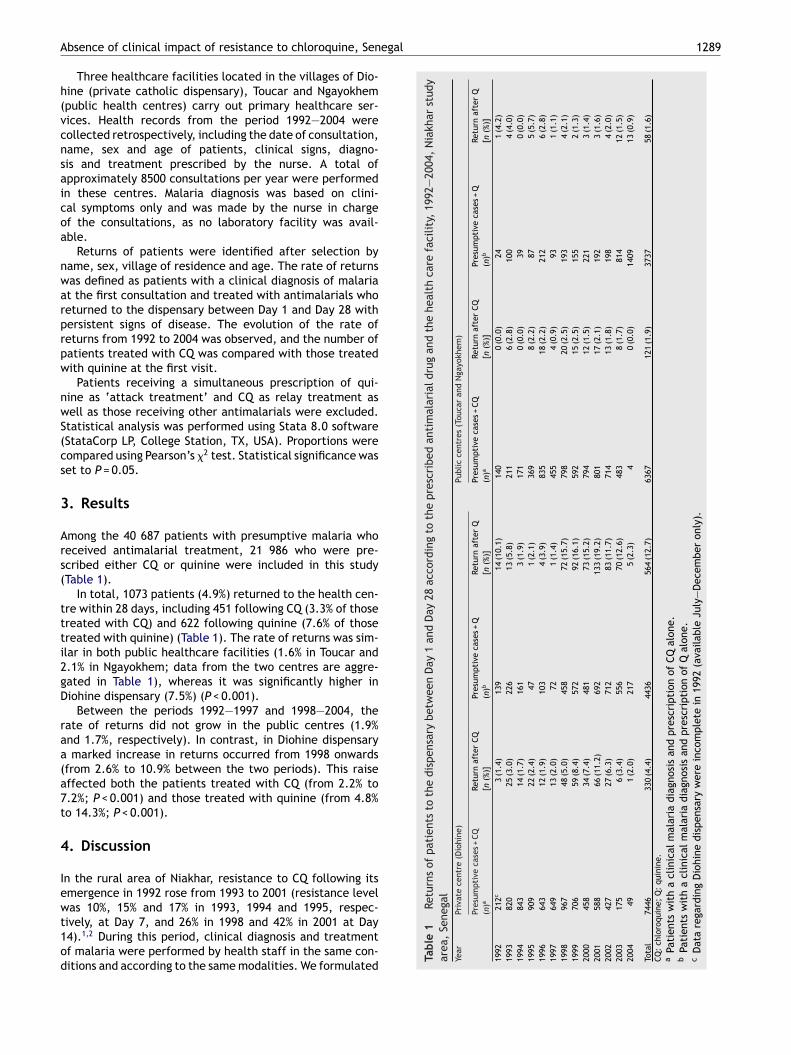
Among the 40 687 patients with presumptive malaria whoreceived antimalarial treatment, 21 986 who were pre-scribed either CQ or quinine were included in this study(Table 1).
In total, 1073 patients (4.9%) returned to the health cen-tre within 28 days, including 451 following CQ (3.3% of thosetreated with CQ) and 622 following quinine (7.6% of thosetreated with quinine) (Table 1). The rate of returns was sim-ilar in both public healthcare facilities (1.6% in Toucar and2.1% in Ngayokhem; data from the two centres are aggre-gated in Table 1), whereas it was significantly higher inDiohine dispensary (7.5%) (P < 0.001).
Between the periods 1992—1997 and 1998—2004, therate of returns did not grow in the public centres (1.9%and 1.7%, respectively). In contrast, in Diohine dispensarya marked increase in returns occurred from 1998 onwards(from 2.6% to 10.9% between the two periods). This raiseaffected both the patients treated with CQ (from 2.2% to7.2%; P < 0.001) and those treated with quinine (from 4.8%to 14.3%; P < 0.001).
4. Discussion
In the rural area of Niakhar, resistance to CQ following itsemergence in 1992 rose from 1993 to 2001 (resistance level
was 10%, 15% and 17% in 1993, 1994 and 1995, respec-tively, at Day 7, and 26% in 1998 and 42% in 2001 at Day14).1,2 During this period, clinical diagnosis and treatmentof malaria were performed by health staff in the same con-ditions and according to the same modalities. We formulatedTabl
e1
Rar
ea,
Sene
gYe
arPr
i
Pre
(n)
1992
219
938
1994
819
959
1996
619
976
1998
919
997
2000
420
015
2002
420
031
2004
Tota
l74
CQ:
chlo
roqu
ina
Pati
ents
wb
Pati
ents
wc
Dat
are
gar

1
tbp
mrsq
swr
2wfalrtsf
rtbr
rtC
AcAm
ap
AamGf
FpuRd
C
E
R
290
he hypothesis that limits and diagnosis errors remained sta-le and resistance to CQ had no impact on diagnosis, butossibly on the efficacy of treatment.
Moreover, CQ has no effect on diseases other thanalaria. Thus, in case of resistance there should be a rise in
eturns of patients who truly suffer from malaria, affectingpecifically the group treated with CQ (in comparison withuinine).
The number of presumptive malaria diagnoses did nothow significant differences during the period of study,hich is not in favour of a possible failure of self-medication
elated to the decreasing efficacy of CQ.In addition, the rate of returns to the health centre within
8 days after treatment did not increase in patients treatedith CQ. In the private dispensary, rates increased three-
old in 1998 but this affected patients treated both by CQnd quinine. This trend was not observed in the two pub-ic centres and we presume that this dramatic increase ofeturns in the private centre was linked to a change of prac-ices from health staff owing to either treatment of patientsuffering from more severe malaria or a higher monitoringollowing quinine injection.
The study of the number of consultations and the rate ofeturns did not give evidence of an increase with time, andhis rate remained very low compared with what would haveeen expected in a region with an established high level ofesistance to CQ.
In contrast to what has been observed with mortalityates during the period 1988—1995,5 there does not appearo be an important rise in morbidity related to the onset ofQ resistance in the area.
uthors’ contributions: All authors participated in the con-eption of the study and interpretation of the results;M collected and analysed the data and drafted theanuscript; AD and JPC revised the article. All authors read
A. Munier et al.
nd approved the final version. JPC is guarantor of theaper.
cknowledgements: The authors would like to thank M. Cotnd P. Arduin for their support, O. Ndiaye for data manage-ent, the US009 Team in Dakar and Niakhar, B.M. Mboup, B.ning and the health staff of Toucar, Diohine and Ngayokhem
or their precious collaboration.
unding: This work was funded by the Institut de rechercheour le développement (IRD, US009 and UR010 researchnits). A.M. was supported by the FRM (Fondation pour laecherche Médicale) and the AFFDU (Association francaisees femmes diplômées des universités).
onflicts of interest: None declared.
thical approval: Not required.
eferences
1. Sokhna CS, Molez JF, Ndiaye P, Sane B, Trape JF. In vivochemosensitivity tests of Plasmodium falciparum to chloroquinein Senegal: the development of resistance and the assess-ment of therapeutic efficacy [in French]. Bull Soc Pathol Exot1997;90:83—9.
2. Gaye O. Surveillance of malaria chemoresistance in Sene-gal. Final report. Dakar, Senegal: Parasitology Unit, UniversityCheikh Anta Diop; 2002.
3. WHO. Susceptibility of Plasmodium falciparum to antimalarialdrugs. Report on global monitoring 1996—2004. Geneva: WorldHealth Organization; 2005.
4. Chippaux JP. The Niakhar study zone in Senegal [in French]. MedTrop (Mars) 2001;61:131—5.
5. Trape JF, Pison G, Preziosi MP, Enel C, Desgrées du Loû A,Delaunay V, et al. Impact of chloroquine resistance on malariamortality. C R Acad Sci III 1998;321:689—97.





![Atelier Inaugural - Datacraft · 2020. 9. 30. · (2013) Machine learning approach for automated screening of malaria parasite using light microscopic images [7] Gopakumar et al](https://img.pdfslide.fr/doc/110x75/60fbf4d22cec0a3b3e4d5e47/atelier-inaugural-datacraft-2020-9-30-2013-machine-learning-approach-for.jpg)














![Burundi Malaria Indicator Survey 2012 [MIS14]](https://img.pdfslide.fr/doc/110x75/586e01031a28abfe5f8b4db9/burundi-malaria-indicator-survey-2012-mis14.jpg)