Embed Size (px)
Citation preview

ASTHMEPréparé par
Nancy Ibrahim R1SUPERVISÉ PAR
DRE. NANHOU
UMF ANNA LABERGE
NOVEMBRE 2010

• Définition• Les facteurs de risque• Physiopathologie • Prévalence et mortalité• Examen physique • Les diagnostics différentiels • Sévérité et contrôle• Investigations et traitement• Pronostic


Définition• L'asthme est un
syndrome clinique caractérisé par:
1.Une obstruction des voies respiratoires épisodiques réversible.
2.L'augmentation de la réactivité bronchique.
3.L'inflammation des voies aériennes.


Les facteurs de risqueAsthme allergique:
- Moulds- Poiles d'animaux- Pollen- Cafard- Dust mites

Les facteurs de risqueAsthme non allergique:
- Certains médicaments (AAS, les bêta-bloquants)- Des produits chimiques, les fumées et les odeurs- Les infections respiratoires virales- Météo (air froid)- Effort physique- La fumée du tabac- La pollution de l'air: le smog


PhysiopathologieLa réponse allergique des voies respiratoires est le résultat
d'une interaction complexe des mast cells, les éosinophiles, les lymphocytes T, macrophages, cellules dendritiques, et des neutrophiles.

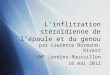
Physiopathologie

PhysiopathologieCliniquement, les manifestations de la
réponse allergique (EAR) dans les voies respiratoires comprennent la constriction bronchique, œdème des voies aériennes, et le mucus plug.
Une réponse tardive allergique peut se produire, qui est caractérisée par une infiltration de cellules inflammatoires dans les voies respiratoires.


PrévalenceSelon WHO, l'asthme est aujourd'hui un sérieux
problème de santé publique avec plus de 100 millions patients dans le monde entier.
Selon Statistique Canada, 8,4% de la population (12 ans et plus) ont été diagnostiqués comme souffrant d'asthme (2000-2001).
L'asthme est la plus fréquente maladie pendant l'enfance et affecte au moins 12% des enfants canadiens.
L'asthme continue d'être une cause majeure d'hospitalisation des enfants au Canada.


Mortalité Au Canada, environ 20 enfants et 500 adultes
meurent chaque année de l’asthme.


Histoire L'histoire classique se compose de:
Wheezing.Toux.Dyspnée.Douleurs à la poitrine .

Histoire Information importants:
* Âge de début * Fréquence et sévérité * Stimulants des symptômes * La variation saisonnière et géographique * Limites de l'activité * Nombre de visites d'urgence * Traitements précédents * Antécédents familiaux d'asthme * Antécédents personnels ou familiaux d'atopie * Symptômes de reflux gastro-œsophagien * L'allergie alimentaire * Courbe de croissance


Examen physiqueL'examen physique est souvent normal.

Examen physiqueTête et cou:
NezSinusVein jugulaireAdénopathies

Examen physiqueCardiaque: Les résultats sont souvent normaux.
Pouls paradoxal > 12 mm HgFréquence cardiaque > 110/min

Examen physiqueRespiratoire:
Fréquence respiratoire > 28/minWheezesL'hyperinflationProlongée phase expiratoireMurmures vésiculaires Signes de détresse respiratoire

Examen physiquePeau: Vérifiez le patient pour la dermatite
atopique.Extrémités


Les diagnostics différentielsMPOC (Emphysème)Mixte des maladies du tissu conjonctif ( Lupus
Érythémateux Dissémine LED, la sclérodermie fibrose des poumons)
Aspergillose (fungale)Bronchiolite (RSV)Embolie pulmonaireBronchiteSarcoïdoseLa bronchite chronique (en particulier le tabagisme)Insuffisance cardiaque congestive et œdème
pulmonaireAspiration de corps étranger

Autres problèmes à prendre en considérationLes enfants et les jeunes adultes
La fibrose kystique Anomalies cardiaques congénitales Anomalies pulmonaires (hamartomes) Pertussis La trachéomalacie Les infections virales

Autres problèmes à prendre en considérationAdultes
Le reflux gastro-œsophagien MPOC / emphysème L'insuffisance cardiaque congestive L'embolie pulmonaire Bronchiectasis Aspiration La fibrose kystique Tumeur endobronchique


InvestigationsLes tests les plus importants sont les tests de
la fonction pulmonaire.Les tests cutanés: radioallergosorbent tests
(RAST), fluorescente allergosorbent tests (FAST).
IgE sériques est élevé.Éosinophilie des expectorations et de sérum.

Les études d'imagerieRadiographies du thorax

Les études d'imagerieModifiée ou limitée scans CT sinus

Les études d'imageriePoitrine tomodensitogrammes

Les études d'imagerieÉchocardiogrammes

Ratio FEV1/FVCObstruction est définie comme un ratio
inférieur à 70% du volume expiratoire maximale première seconde(VEMS) de la capacité vitale forcée (CVF).
VEMS est normalement supérieure à 80% des valeurs prédites par l'âge.

Test de provocation à la méthacholine

Mesure d'oxygénationC'est à dire avec l'oxymétrie de pouls artériel
ou analyse des gaz du sang.

Les résultats histologiquesCorps Creola

Les résultats histologiquesLes cristaux de Charcot-Leyden

Les résultats histologiquesSpirales de Curschmann


SévéritéClassify severity at presentation
Intermittent
Mild Moderate Severe
Category 1 2 3 4
Daytime symptoms ≤ 2 / week
2 – 4 / week
> 4 / week
Continuous
Night-time symptoms ≤ 1/month
2 -4/month
> 4 / month
Frequent
FEV 1 ≥ 80 % 60 – 80 % 40 – 60 % < 40 %

Contrôle* Bien contrôlée * Pas bien contrôlée * Très mal contrôlés


Les soins médicaux Les objectifs du traitement:
Réduire les symptômes.Améliorer la qualité de vie.Réduire le besoin de soins d'urgence ou des
hospitalisations.Normaliser les résultats des tests de fonction
pulmonaires.Diminuer le processus inflammatoire.

Les soins médicaux Pharmacothérapie Contrôle de l'environnementL'immunothérapie allergéniqueLes anticorps contre IgEL'éducation


PharmacothérapieІ- β2-agonistes à courte durée d’action:
Salbutamol (Ventolin) Terbutaline
β2 agonistes à courte durée, au besoin, sont les plus efficaces pour le soulagement rapide des symptômes d'asthme.

PharmacothérapieІІ- Antileucotriènes
Montélukast Zafirlukast

PharmacothérapieІІІ- Cromoglycates:
Nédocromil synchron – nébuliseur Cromoglycate de sodium

PharmacothérapieІѴ- Corticoïdes topiques
a) Corticoïdes topiques Fluticasone (Flovent) Budésonide
b) Corticoïdes topiques + β2-agonistes Fluticasone + Salmétérol (Advair) Budésonide + Formotérol (Symbicort)Toujours utiliser en bithérapie

PharmacothérapieѴ- β2-agonistes à longue durée d’action a) β2-agonistes
FormotérolSalmétérol (Serevent)
b) β2-agonistes + Corticoïdes topiques

PharmacothérapieѴІ- Xanthines (Théophylline)

PharmacothérapieѴІІ- Corticoïdes systemiques
iv: Méthylprednisolonepo: Prednisone

• Short-acting β2 agonist as needed (reliever)• Environmental control• Education / self management
Step 1 : Intermittent
Step 2 : Mild persistent
Step 3 : Moderate persistent
Step 4 : Severe persistent
• No daily preventer or controller medication needed
Daily medication•Low-dose inhaled corticosteroid•Secondary options:
• Cromoglycate/Nedocromil• Sustained release theophylline• Leukotriene receptor antagonist
Daily medication•Medium-dose inhaled corticosteroid•And if needed:
• Long-acting inhaled β2 agonist or sustained release theophylline
• Consider adding leukotriene receptor antagonist
Daily medication•High-dose inhaled corticosteroid•And if needed
• Long-acting inhaled β2 agonist or sustained release theophylline
• Consider adding leukotriene receptor antagonistIf still not controlled•Add prednisone long-term (preferably alternate days) – reduce to lowest dose that controls symptoms

Choice of spacer device:
Increase treatment•If control is not achieved, consider step up. First review medication technique, adherence and environmental control.•A short course of oral steroids may be required to achieve control (prednisone 1-2 mg/kg/day for 7-14 days)
Reduce treatment•Review treatment every 3-6 months. If control is sustained reduce treatment.
< 3 yrs MDI + spacer with mask> 3 yrs MDI + spacer with mouth piece


Autres soins ambulatoiresRéévaluer la sévérité, la compliance et la
réponse au traitement.Questionnaires. http://www.asthmacontrol.com
Assurer l'évitement de l'environnement.Visite à domicile.Modifier les doses au besoin.


Éviter les allergènes


ImmunothérapieDes injections répétées de petites doses
d'allergènes


ConsultationsConsulter un pneumologue, allergiste/immunologiste, ou les deux.


ActivitéMaintenir l'activité physique et l'exercice est
essentiel

ActivitéPlusieurs études récentes ont démontré que
la pratique régulière de la capacité aérobie et la perte de poids peut améliorer la physiologie des voies aériennes et la dyspnée.


Éducation du patient Programmes d'éducation adéquats pour les
parents et / ou les patients sont les suivantes: La description des maladies asthme.Identification et contrôle des irritants
environnementaux.L'utilisation adéquate des médicaments.Les symptômes allergiques des voies
respiratoires supérieures peuvent alerter d’avoir l'asthme au future.


PronosticLes signes qui peuvent indiquer un mauvais
pronostic :Exacerbations sévères.Plus de 2 β2-agonistes à courte durée d’action
par mois.La dépendance des glucocorticoïdes.Comorbidités médicaux importantes.La maladie psychiatrique.La consommation de drogues.


ConclusionL'asthme est la plus fréquente maladie
pendant l'enfance.L'examen physique est souvent normal,
l’histoire est le plus important. Les tests les plus importants sont les tests de
la fonction pulmonaire.Le but est d’améliorer la qualité de vie.Modifier les doses au besoin.Éducation des patients est très importante.

BiographieWHO Fact Sheet No206Canadian Lung Association.Statistics Canada. Millar, Wayne J. and Gerry B. Hill.
Childhood Asthma, Health Reports, Vol. 10, No. 3Asthma society of CanadaNelson HSAllergen immunotherapy: where is it now?. J Allergy
Clin Immunol. Apr 2007http://emedicine.medscape.comMedcine interne - Philippe Furger