Embed Size (px)
Citation preview
Immuno-analyse et biologie spécialisée (2012) 27, 97—103
Disponible en ligne sur
www.sciencedirect.com
REVUES GÉNÉRALES ET ANALYSES PROSPECTIVES
Effects of dietetic WHO’s recommendations on HDL-Clevel in a Tunisian obese groupLes effets des recommandations diététiques de l’OMS sur le niveau deHDL-C dans un groupe tunisien d’obèses
I. Boumaizaa, S. Berriri a, A. Omezzinea, L. Rebhia, J. Rejeba,N. Ben Rejeba, N. Nabli a, A. Ben Abdellazizb, A. Bouslamaa,∗
a Biochemistry department, UR MSP 28/04, Sahloul University Hospital, 4054 Sousse, Tunisiab Information System Direction, Sahloul University Hospital, Sousse, Tunisia
Received 7 June 2011; accepted 20 February 2012
KEYWORDSHDL cholesterol;WHO’srecommendations;Dietetic;Fatty acids
SummaryObjective. — Evaluate the effect of dietetic WHO’s recommendations on hypoHDLemia in obeseTunisians volunteers.Methods. — We enrolled 93 volunteers hospital personal. Anthropometric parameters, bloodpressure, lipids levels, glycemia and insulinemia were measured. Dietary intake assessmentwas undertaken, results were transformed into dichotomic variables according to the respector not of the WHO’s recommendations for chronic diseases prevention. Health Diet Index (HDI)was calculated.Results. — After adjustment for potential confounders factors, we found significant reductionof hypoHDLemia risk by respect of the dietetic WHO’s recommendations for the saturated fattyacids (OR = 0.602; P = 0.033), monounsaturated fatty acids (OR = 0.765; P = 0.038), fish consump-tion (OR = 0.633; P = 0.049) free sugar (OR = 0.759; P = 0.041). OR of hypoHDLemia associatedwith a HDI greater than or equal to 4 was 0.218; P = 0.048. These same recommendationshave significant effect to reduce high TC/HDL-C. In addition PUFA [6—10%], total carbohydrates
[55—75%] and increased fruits and vegetables protect against high TC/HDL-C.Conclusion. — Several dietetic WHO’s recommendations seem to prevent hypoHDLemia. Theassociation of at least four recommendations had a significant beneficial effect.. All rights reserved.
© 2012 Elsevier Masson SAS∗ Corresponding author.E-mail address: [email protected] (A. Bouslama).
0923-2532/$ – see front matter © 2012 Elsevier Masson SAS. All rights reserved.doi:10.1016/j.immbio.2012.02.006

98 I. Boumaiza et al.
MOTS CLÉSHDL-C ;Les recommandationsOMS ;Diététique ;Acides gras
RésuméObjectif. — Évaluez l’effet de diététique selon l’OMS sur l’hypoHDLemie chez des volontairesTunisiens obèses.Méthodes. — Nous avons recruté 93 personnels volontaires de l’hôpital. Les paramètres anthro-pométriques, la prise de tension, la concentration des lipides, la glycémie et l’insulinémie ontété mesurés. La consommation diététique a été évaluée, les résultats ont été transformés àdes variables dichotomiques selon le respect ou pas des recommandations de l’OMS pour laprévention des maladies chroniques.Résultats. — Après ajustement aux facteurs confondants, nous avons trouvé la réduction signi-ficative de risque d’hypoHDLemie en respectant les recommandations diététiques de l’OMSpour les acides gras saturés (OR = 0,602 ; p = 0,033), acides gras mono-insaturés (OR = 0,765 ;p = 0,038), consommation de poisson (OR = 0,633 ; p = 0,049) sucres simples (OR = 0,759 ;p = 0,041). OR de l’hypoHDLemie associé à un HDI supérieur ou égal à 4 était 0,218 ; p = 0,048.Ces mêmes recommandations ont un effet significatif pour réduire l’augmentation du rap-port CT/HDL-C. En plus, les acides gras poly-insaturés [6—10 %], les sucres totaux [55—75 %]et l’augmentation des fruits et des légumes protègent contre l’élévation du rapport CT/HDL-C.Conclusion. — Plusieurs recommandations diététiques de l’OMS semblent empêcherl’hypoHDLemie. L’association d’au moins quatre recommandations avait un effet protecteursignificatif.
. Tou
I
Ri‘ci(
abarftb
cfiqsen
d(Hii
apc
thbv
CdTt2oao
bcatC
aCT
M
TU
S
WowweA
viewed by a structured questionnaire for the informations
© 2012 Elsevier Masson SAS
ntroduction
esults of prospective observational studies, controlled clin-cal trials with drugs, mechanistic studies, and genetic‘experiments of nature’’ all strongly suggest that high con-entrations of high density lipoprotein cholesterol (HDL-C)n the circulation help to prevent coronary artery diseaseCAD) and other cardiovascular diseases (CVD) [1—5].
HDL is a heterogeneous group of particles composed of core of cholesteryl ester and triglycerides surroundedy an amphipathic layer of free cholesterol, phospholipidsnd apolipoproteins [6,7]. They are key players in theeverse cholesterol transport, which shuttles cholesterolrom peripheral cells (e.g. macrophages) to the liver or otherissues [8]. This complex process is thought to represent theasis for the antiatherogenic properties of HDL particles [4].
Abdominal obesity is associated with a decreased plasmaoncentration of HDL cholesterol and with qualitative modi-cations of HDL, such as triglyceride enrichment. Because ofuantitative and qualitative modifications, HDL from obeseubjects may be less protective against impairments ofndothelium-dependent vaso-relaxation than HDL from leanormolipidemic subjects [9,10].
Diet, in addition to various other factors, such as gen-er, menopausal status, hormone therapy, body mass indexBMI), exercise, smoking, and alcohol intake, can influenceDL-C concentrations [11]. The interplay between genet-
cs and environmental factors, such as diet, may be of keymportance in determining HDL levels [12].
Dietary macronutrient composition, particularly the bal-nce among carbohydrate, protein, and fat, as well as thearticular fatty acid composition of the diet, affects HDL-Concentrations [13].
A large number of dietary factors have been linkedo CVD. In fact, unhealthy dietary practices include the
igh consumption of saturated fats, salt and refined car-ohydrates, as well as low consumption of fruits andegetables, and these tend to cluster together to increaseoha
s droits réservés.
VD risk [14]. Public health organizations worldwide pro-uced dietary guidelines to help reduce the risk of CVD.he World Health Organization (WHO)/Food and Agricul-ure Organization (FAO) expert consultation report (Geneva,003) is typical and recommends increasing the consumptionf fruits and vegetables, increasing the consumption of fish,nd to alter the types of fats and oils, as well as the amountf sugars and starch consumed [14].
The effects of dietary on the risk of CAD have traditionallyeen estimated from their effects on low density lipoproteinholesterol (LDL-C). However, dietary, also affect HDL-C,nd atherogenicity cholesterol ratio: total to HDL choles-erol ratio (TC/HDL-C), which is a more specific marker ofVD than is LDL-C [15].
The aim of this study is to evaluate the effect of thepplication of the dietetic WHO’s recommendations on HDL-
and on the atherogenicity cholesterol ratio in a group ofunisian obese volunteers.
aterials and methods
he study was approved by the ethics committee of theniversity Hospital Sahloul, Tunisia.
ubjects
e recruited 93 personal volunteers obese (BMI ≥ 30 Kg/m2)f university hospital Sahloul, Sousse (a coastal region). Ageas 23 to 61 years, sex ratio was 0.27. Exclusion criteriaere dysthyroïdia, hepatic, gastrointestinal or kidney dis-ases, and lipids lowering drugs intake familial dyslipidemia.ll volunteers provided informed consent.
All of the study participants were individually inter-
n sociodemographic characteristics, details of personalistory, presence of disease, drug intake if any, smokingnd alcohol habits. We divided studied population in two

Diet and HDL-C
Table 1 Dietary WHO’s recommendations for prevention ofCAD [14].
Food items Objective (% otherwisespecified)
Total fat 15—30Saturated fatty acids < 10Polyunsaturated fatty acids 6—10Monounsaturated fatty acids >15Total carbohydrate 55—75Free sugar < 10Proteins 10—15Fruits and vegetables ≥ 400 g/dayFibers ≥ 25 g/dayFish ≥ 2/week
jTs
B
Boemc4do
Cg
ir
D
Dti1[oe1i
S
STmsdvtcamt
f
R
C
Am(HDL-C < 1.29 mmol/L in women and < 1.03 mmol/L in men)
WHO: World Health Organization; CAD: cardiovascular disease.
groups with and without hypoHDLemia: HDL-C less than1.29 mmol/L in women and less than 1.03 mmol/L in men[16].
Assessment of dietary intake
Subjects were interviewed privately, face to face; trainedinterviewers using pretested questionnaires conducted theinterviews. Dietary intake assessment was undertaken with3 days recalls as described by Moshfegh et al. [17]. Two dayswere selected randomly from the weekdays, the third onefrom the weekend. Standard reference tables were used toconvert household portions to grams for computerization.After coding of diaries, the dietary recall form was linked toa nutrient database (Dietetik® designed for Tunisian foodsand Nutrilog®) and daily energy and nutrient intakes (car-bohydrates, proteins, and fats) for each individual weredetermined from the means of the dietary recalls.
Intakes of macronutrients were presented as a percent-age of energy intakes. The results were transformed intodichotomic variables according to the respect or not of theWHO’s recommendations (Table 1) [14]. The group of food ormacronutrient was coded by 1 for recommendation respectand 0 for contrary case.
A Healthy Diet Index (HDI) to evaluate cumulate effectof the recommendations was calculated for each individ-ual as described by Boylan et al., 2009 [18]. It is the sumof seven dichotomic variables which are based on differ-ent aspects of a healthful food: saturated fatty acids (SFA),polyunsaturated fatty acids (PUFA), complex carbohydratesand free sugar, proteins, fruits and vegetables (g/day) andfibers (g/day). This index varies between 0 and 7. We omit-ted from the HDI, total fat and total glucids to avoid theoverlapping between categories.
Anthropometric parameters and blood pressure measure-ment, weight and height were measured on the subjectsbarefooted and lightly clothed. BMI was calculated as bodyweight (kg)/height2 (m)2 and obesity was defined as BMIgreater than or equal to 30 kg/m2 [19].
Waist circumference was measured by trained examinerfrom the narrowest point between the lower borders of therib cage and the iliac crest.
(dh
99
Blood pressure was read from the left arm of seated sub-ects with a blood pressure monitor after 20 min of rest.he two last measurements average was recorded for eachubject.
iochemical measurements
lood samples were collected from subjects after 12 hvernight fast. Serum total cholesterol (TC) and triglyc-rides (TG) were determined by standard assays. HDL-C waseasured by direct assay. LDL-C concentrations were cal-
ulated with the Friedwald formula [20], if TG less than mmol/L. If not, LDL-C concentrations were measured byirect assay. Fasting glucose was measured by the glucosexidase method.
All biochemical parameters were performed on SynckromX7 Clinical System (Beckman, Fullerton, CA, USA). Athero-enicity cholesterol ratio: TC/HDL-C was calculated.
Insulin concentrations were measured by microparticulemmuno-assay (MEIA) on AxSym® Abbott (Abbott laborato-ies, Abbott Parck, IL 60064).
efinitions of risk factors
iabetes mellitus was defined as fasting glucose morehan 7 mmol/L or currently receiving anti diabetic med-cation [21]. Hypertension was defined as greater than40/90 mmHg of currently or antihypertensive medication22]. Dyslipidemia was defined as LDL-C concentration morer equal to 4.1 mmoL/L and or HDL-C concentration less orqual to 1 mmoL/L and or TG concentration more or equal to.71 mmoL/L [23]. Metabolic syndrome was defined accord-ng to the IDF definition [24].
tatistical methods
tatistical analyses were performed by SPSS 16.0.he biological parameters values were reported aseans ± standard deviation (S.D) and were compared by
tudent’s t test. The parameters not having a Gaussianistribution were logarithmically transformed. Categoricalariables were analyzed by the Chi2 test. Odds ratio (OR),wo-tailed P-values and 95% confidence interval (CI) werealculated as a measure of the association of hypoHDLemiand high cholesterol/HDL-C ratio with several WHO’s recom-endation. OR were adjusted by logistic binary regression
o confounders parameters and to other food items.A P value of < 0.05 was considered statistically significant
or all tests.
esults
linical and biochemical characteristics
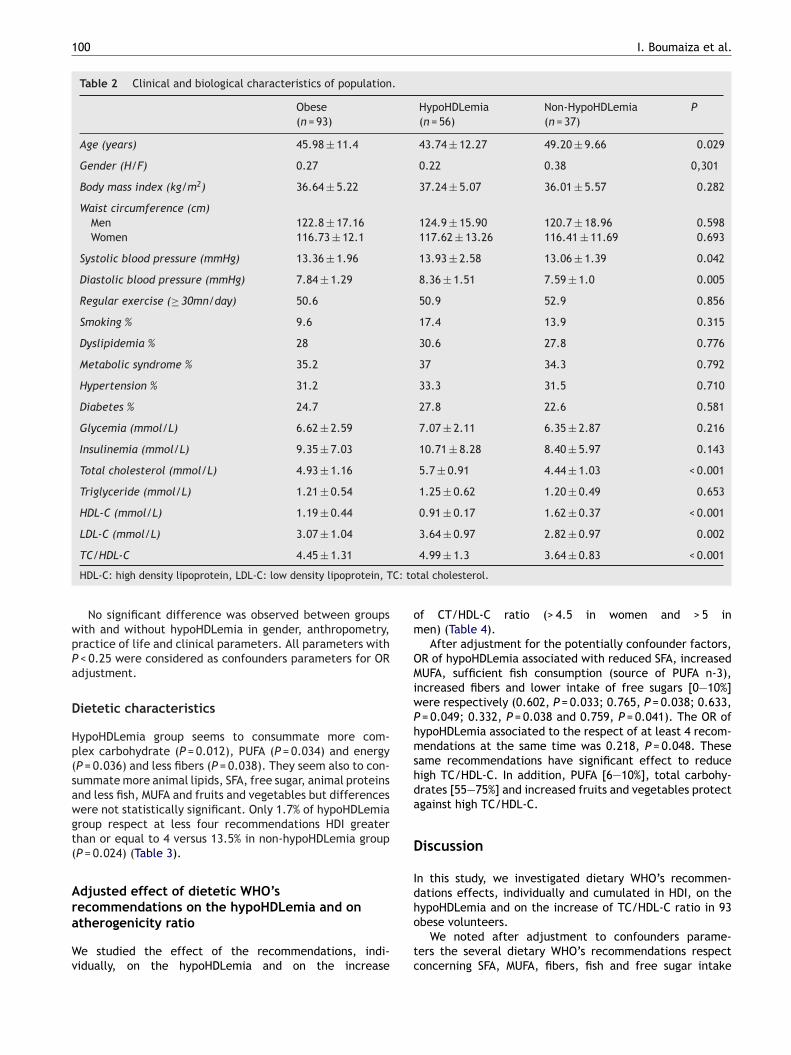
mong the 93 obese volunteers (sex ratio = 0.27,ean age = 45.98 ± 11.4), 60% were with hypoHDLemia
Table 2). HypoHDLemia group had higher systolic andiastolic blood pressure, higher TC and LDL-C levels andigher TC/HDL-C ratio.
100 I. Boumaiza et al.
Table 2 Clinical and biological characteristics of population.
Obese(n = 93)
HypoHDLemia(n = 56)
Non-HypoHDLemia(n = 37)
P
Age (years) 45.98 ± 11.4 43.74 ± 12.27 49.20 ± 9.66 0.029
Gender (H/F) 0.27 0.22 0.38 0,301
Body mass index (kg/m2) 36.64 ± 5.22 37.24 ± 5.07 36.01 ± 5.57 0.282
Waist circumference (cm)Men 122.8 ± 17.16 124.9 ± 15.90 120.7 ± 18.96 0.598Women 116.73 ± 12.1 117.62 ± 13.26 116.41 ± 11.69 0.693
Systolic blood pressure (mmHg) 13.36 ± 1.96 13.93 ± 2.58 13.06 ± 1.39 0.042
Diastolic blood pressure (mmHg) 7.84 ± 1.29 8.36 ± 1.51 7.59 ± 1.0 0.005
Regular exercise (≥ 30mn/day) 50.6 50.9 52.9 0.856
Smoking % 9.6 17.4 13.9 0.315
Dyslipidemia % 28 30.6 27.8 0.776
Metabolic syndrome % 35.2 37 34.3 0.792
Hypertension % 31.2 33.3 31.5 0.710
Diabetes % 24.7 27.8 22.6 0.581
Glycemia (mmol/L) 6.62 ± 2.59 7.07 ± 2.11 6.35 ± 2.87 0.216
Insulinemia (mmol/L) 9.35 ± 7.03 10.71 ± 8.28 8.40 ± 5.97 0.143
Total cholesterol (mmol/L) 4.93 ± 1.16 5.7 ± 0.91 4.44 ± 1.03 < 0.001
Triglyceride (mmol/L) 1.21 ± 0.54 1.25 ± 0.62 1.20 ± 0.49 0.653
HDL-C (mmol/L) 1.19 ± 0.44 0.91 ± 0.17 1.62 ± 0.37 < 0.001
LDL-C (mmol/L) 3.07 ± 1.04 3.64 ± 0.97 2.82 ± 0.97 0.002
C: to
wpPa
D
Hp(sawgt(
Ara
Wv
om
OMiwPhmshda
D
Idh
TC/HDL-C 4.45 ± 1.31
HDL-C: high density lipoprotein, LDL-C: low density lipoprotein, T
No significant difference was observed between groupsith and without hypoHDLemia in gender, anthropometry,ractice of life and clinical parameters. All parameters with
< 0.25 were considered as confounders parameters for ORdjustment.
ietetic characteristics
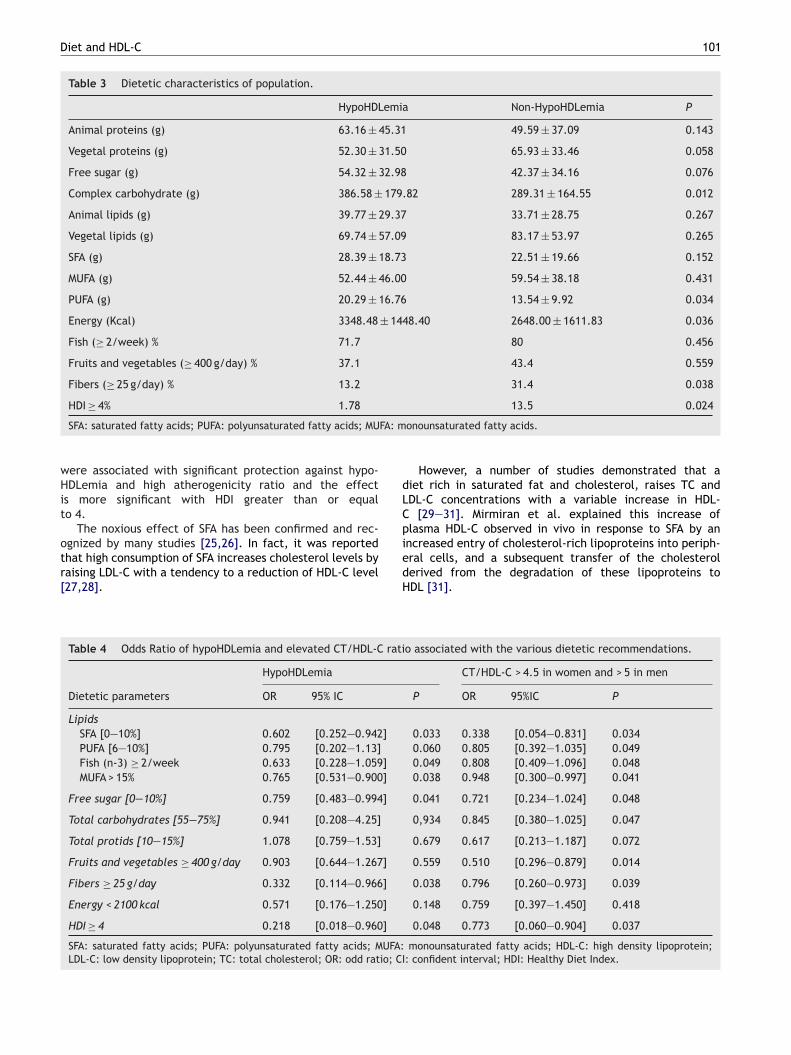
ypoHDLemia group seems to consummate more com-lex carbohydrate (P = 0.012), PUFA (P = 0.034) and energyP = 0.036) and less fibers (P = 0.038). They seem also to con-ummate more animal lipids, SFA, free sugar, animal proteinsnd less fish, MUFA and fruits and vegetables but differencesere not statistically significant. Only 1.7% of hypoHDLemiaroup respect at less four recommendations HDI greaterhan or equal to 4 versus 13.5% in non-hypoHDLemia groupP = 0.024) (Table 3).
djusted effect of dietetic WHO’secommendations on the hypoHDLemia and on
therogenicity ratioe studied the effect of the recommendations, indi-idually, on the hypoHDLemia and on the increase
o
tc
4.99 ± 1.3 3.64 ± 0.83 < 0.001
tal cholesterol.
f CT/HDL-C ratio (> 4.5 in women and > 5 inen) (Table 4).After adjustment for the potentially confounder factors,
R of hypoHDLemia associated with reduced SFA, increasedUFA, sufficient fish consumption (source of PUFA n-3),
ncreased fibers and lower intake of free sugars [0—10%]ere respectively (0.602, P = 0.033; 0.765, P = 0.038; 0.633,
= 0.049; 0.332, P = 0.038 and 0.759, P = 0.041). The OR ofypoHDLemia associated to the respect of at least 4 recom-endations at the same time was 0.218, P = 0.048. These
ame recommendations have significant effect to reduceigh TC/HDL-C. In addition, PUFA [6—10%], total carbohy-rates [55—75%] and increased fruits and vegetables protectgainst high TC/HDL-C.
iscussion
n this study, we investigated dietary WHO’s recommen-ations effects, individually and cumulated in HDI, on theypoHDLemia and on the increase of TC/HDL-C ratio in 93
bese volunteers.We noted after adjustment to confounders parame-ers the several dietary WHO’s recommendations respectoncerning SFA, MUFA, fibers, fish and free sugar intake
Diet and HDL-C 101
Table 3 Dietetic characteristics of population.
HypoHDLemia Non-HypoHDLemia P
Animal proteins (g) 63.16 ± 45.31 49.59 ± 37.09 0.143
Vegetal proteins (g) 52.30 ± 31.50 65.93 ± 33.46 0.058
Free sugar (g) 54.32 ± 32.98 42.37 ± 34.16 0.076
Complex carbohydrate (g) 386.58 ± 179.82 289.31 ± 164.55 0.012
Animal lipids (g) 39.77 ± 29.37 33.71 ± 28.75 0.267
Vegetal lipids (g) 69.74 ± 57.09 83.17 ± 53.97 0.265
SFA (g) 28.39 ± 18.73 22.51 ± 19.66 0.152
MUFA (g) 52.44 ± 46.00 59.54 ± 38.18 0.431
PUFA (g) 20.29 ± 16.76 13.54 ± 9.92 0.034
Energy (Kcal) 3348.48 ± 1448.40 2648.00 ± 1611.83 0.036
Fish (≥ 2/week) % 71.7 80 0.456
Fruits and vegetables (≥ 400 g/day) % 37.1 43.4 0.559
Fibers (≥ 25 g/day) % 13.2 31.4 0.038
HDI ≥ 4% 1.78 13.5 0.024
FA: m
dLCpi
SFA: saturated fatty acids; PUFA: polyunsaturated fatty acids; MU
were associated with significant protection against hypo-HDLemia and high atherogenicity ratio and the effectis more significant with HDI greater than or equalto 4.
The noxious effect of SFA has been confirmed and rec-ognized by many studies [25,26]. In fact, it was reported
that high consumption of SFA increases cholesterol levels byraising LDL-C with a tendency to a reduction of HDL-C level[27,28].edH
Table 4 Odds Ratio of hypoHDLemia and elevated CT/HDL-C rati
HypoHDLemia
Dietetic parameters OR 95% IC
LipidsSFA [0—10%] 0.602 [0.252—0.942]
PUFA [6—10%] 0.795 [0.202—1.13]
Fish (n-3) ≥ 2/week 0.633 [0.228—1.059]
MUFA > 15% 0.765 [0.531—0.900]
Free sugar [0—10%] 0.759 [0.483—0.994]
Total carbohydrates [55—75%] 0.941 [0.208—4.25]
Total protids [10—15%] 1.078 [0.759—1.53]
Fruits and vegetables ≥ 400 g/day 0.903 [0.644—1.267]
Fibers ≥ 25 g/day 0.332 [0.114—0.966]
Energy < 2100 kcal 0.571 [0.176—1.250]
HDI ≥ 4 0.218 [0.018—0.960]
SFA: saturated fatty acids; PUFA: polyunsaturated fatty acids; MUFA:LDL-C: low density lipoprotein; TC: total cholesterol; OR: odd ratio; CI
onounsaturated fatty acids.
However, a number of studies demonstrated that aiet rich in saturated fat and cholesterol, raises TC andDL-C concentrations with a variable increase in HDL-
[29—31]. Mirmiran et al. explained this increase oflasma HDL-C observed in vivo in response to SFA by anncreased entry of cholesterol-rich lipoproteins into periph-
ral cells, and a subsequent transfer of the cholesterolerived from the degradation of these lipoproteins toDL [31].o associated with the various dietetic recommendations.
CT/HDL-C > 4.5 in women and > 5 in men
P OR 95%IC P
0.033 0.338 [0.054—0.831] 0.0340.060 0.805 [0.392—1.035] 0.0490.049 0.808 [0.409—1.096] 0.0480.038 0.948 [0.300—0.997] 0.041
0.041 0.721 [0.234—1.024] 0.048
0,934 0.845 [0.380—1.025] 0.047
0.679 0.617 [0.213—1.187] 0.072
0.559 0.510 [0.296—0.879] 0.014
0.038 0.796 [0.260—0.973] 0.039
0.148 0.759 [0.397—1.450] 0.418
0.048 0.773 [0.060—0.904] 0.037
monounsaturated fatty acids; HDL-C: high density lipoprotein;: confident interval; HDI: Healthy Diet Index.

1
wicttbM
PSat
i7nsCNcC
PstSMo[dlerL
retmiptL
sMt
fiere
C
Rsret
ta
D
Tc
A
Toteh
att
TaWp
R
[
02
Public health emphasis on reducing SFA consumptionithout considering the replacement nutrient or, more
mportantly, the many other food-based risk factors forardiometabolic diseases is unlikely to produce substan-ial intended benefits [25]. A key question is whethero reduce SFA intakes via low-fat, high-complex car-ohydrate or by moderate-fat diets rich in PUFA orUFA.
In our study, we noted that recommendation concerningUFA seems to protect mainly against high TC/HDL-C ratio.tudies about PUFA effect on lipid profile were controversialnd this was probably related to different effect accordingheir nature, omega 6 or omega 3 [15].
Sousse is a coastal region, that’s why 74.4% of our stud-ed population had sufficient fish consumption, respectively1.7% and 80% in groups with and without hypoHDLemia. Weoted that consumption of fish, more than twice a week,eems to reduce the frequency of hypoHDLemia and of highT/HDL-C ratio. Baik et al. reported the same result [32].umerous large prospective cohort studies have shown aonsistent inverse association between fish intake and fatalHD [33].
Lowering of HDL-C levels by high amounts of dietaryUFA is usually considered as unfavorable. For this rea-on, MUFA has gained interest. In our study, MUFA seemso protect against hypoHDLemia and high TC/HDL-C ratio.ome studies have provided evidence that diets high inUFA such as a Mediterranean diet may reduce the riskf CAD by improving insulin sensitivity and serum lipids34—36]. Bos et al. reported that replacing a high SFA-iet with a high MUFA or a Mediterranean improved serumipid [35]. MUFA seems to induce synthesis of lipoproteinsasily recognized by the lipoprotein lipase, leading to TGeduction, HDL-C increase and an efficient clearance ofDL-C [37].
Concerning carbohydrate, our results suggest that aeduction in free sugar intake [0—10%], has a beneficialffect on hypoHDLemia and CT/HDL-C ratio and a reduc-ion in total carbohydrate [55—75%] have a beneficial effectainly on CT/HDL-C. It was reported that an increased
ntake in carbohydrates has a negative effect on lipidsarameters proportionally to the glycemic index [15] andhat lowering glycemic index enhanced reduction in TC andDL-C concentrations [38].
The effect of the replacement of SFA with carbohydrateeems to be uncertain [38]. Clifton et al. found that a highUFA diet produced a significantly better lipoprotein profil
han a high carbohydrate diet [39].Our results suggest that a higher consumption in
bers greater than or equal 25 g/day has a beneficialffect on hypoHDLemia and CT/HDL-C ratio. The sameesults were reported by Jenkins et al. and Mirmirant al. [40,41].
onclusion
eplacement of SFA by MUFA, sufficient fish and fibers con-
umption and reduced free sugar diet according to WHO’secommendations seem to have a significant protectiveffect on hypoHDLemia and on high TC/HDL-C ratio. Tunisianraditional dietetic habits similar to Mediterranean standard[
I. Boumaiza et al.
raditional food could be the best alternative in order to takeccount of all WHO’s measurements.
isclosure of interest
he authors declare that they have no conflicts of interestoncerning this article.
cknowledgements
his study was supported by grants from the Tunisian Ministryf Higher Education, Scientific Research and Technology andhe Tunisian Ministry of Health (UR 28/04); without theirxtremely generous and strong support, this study could notave been undertaken.
We are especially grateful to the study participants. Wecknowledge general director of Sahloul University Hospi-al and the excellent technical assistance of members ofhe Biochemistry Department of Sahloul University Hospital.
Funding: this study was supported by grants from theunisian ministry of Higher education, scientific researchnd technology and the ministry of health (UR 28/04).ithout their extremely generous and strong support, this
roject would not have happened.
eferences
[1] Kitamura A, Iso H, Naito Y, et al. High-density lipoproteincholesterol and premature coronary heart disease in urbanJapanese men. Circulation 1994;89:2533—9.
[2] Stein O, Stein Y. Atheroprotective mechanisms of HDL.Atherosclerosis 1999;144:285—301.
[3] Plump AS, Scott CJ, Breslow JL. Human apolipoprotein A-I geneexpression increases high density lipoprotein and suppressesatherosclerosis in the apolipoprotein E-deficient mouse. ProcNatl Acad Sci USA 1994;91:9607—11.
[4] Kontush A, Chapman MJ. Functionally defective high-densitylipoprotein: a new therapeutic target at the crossroads of dys-lipidemia, inflammation, and atherosclerosis. Pharmacol Rev2006;58:342—74.
[5] Rubins HB, Robins SJ, Collins D, et al. Gemfibrozil for the sec-ondary prevention of coronary heart disease in men with lowlevels of high-density lipoprotein cholesterol. N Engl J Med1999;341:410—8.
[6] Gotto Jr AM. Recent studies on the structure of human serumlow-and high-density lipoproteins. Proc Natl Acad Sci U S A1969;64(3):1119—27.
[7] Camejo G. The structure of the high density lipoproteins ofthe plasma: various properties of its protein component. ActaCient Venez 1972;23:5—10.
[8] Bruce C, Chouinard Jr RA, Tall AR. Plasma lipid transferproteins, high density lipoproteins, and reverse cholesteroltransport. Annu Rev Nutr 1998;18:297—330.
[9] Perseıgol L, Verge ‘s B, Gambert P, Duvillard L. Inabilityof HDL from abdominally obese subjects to counteract theinhibitory effect of oxidized LDL on vasorelaxation. J Lipid Res2007;48:1396—401.
10] Mooradian AD, Haas MJ, Wehmeier KR, Wong NCW. Obesity-
related changes in high-density lipoprotein metabolism. RevIntegr Physiol 2008;6:1152—60.11] Grundy SM, Denke MA. Dietary influences on serum lipids andlipoproteins. J Lipid Res 1990;31:1149—72.
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
Diet and HDL-C
[12] Lu Y, Feskens EJ, Dollé ME, et al. Dietary n-3 and n-6polyunsaturated fatty acid intake interacts with FADS1 geneticvariation to affect total and HDL-cholesterol concentrationsin the Doetinchem Cohort Study. Am J Clin Nutr 2010;92(1):258—65.
[13] Hill AM, Kris-Etherton PM. Contemporary strategies for weightloss and cardiovascular disease risk factor modification. CurrAtheroscler Rep 2008;10(6):486—96.
[14] World Health Organization: diet nutrition and the preventionof chronic diseases. World Health Organization; 2003.
[15] Mensink RP, Zock PL, Kester ADM, Katan MB. Effects of dietaryfatty acids and carbohydrates on the ratio of serum totalto HDL cholesterol and on serum lipids and apolipoproteins:a meta-analysis of 60 controlled trials 1-3. Am J Clin Nutr2003;77:1146—55.
[16] Alberti KG, Zimmet P, Shaw J. The metabolic syndrome-a newworldwide definition. Lancet 2005;366:1059—62.
[17] Moshfegh AJ, Rhodes DG, Baer DJ, Murayi T, Clemens JC, Rum-pler WV, et al. The US Department of Agriculture AutomatedMultiple-Pass Method reduces bias in the collection of energyintakes. Am J Clin Nutr 2008;88:324—32.
[18] Boylan S, Welch A, Pikhart H, et al. Diatary habits in threecentral and eastern European countries: the Happiees study.BMC Public Health 2009;1(9):439.
[19] World Health Organisation. Physical status: the use andinterpretation anthropometry: report of a WHO Expert Com-mittee, WHO Technical Report Series. Geneva: WHO 1995:854;321—44.
[20] Friedewald WT, Levy RI, Fredrickson DS. Estimation of theconcentration of low-density lipoprotein cholesterol in plasma,without use of the preparative ultracentrifuge. Clin Chem1972;18:499—502.
[21] Alberti KG, Zimmet PZ. Definition, diagnosis and classi-fication of diabetes mellitus and its complications. Part1: diagnosis and classification of diabetes mellitus provi-sional report of a WHO consultation. Diabet Med 1998;15:539—53.
[22] Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA,Izzo Jr JL, et al. Seventh Report of the Joint National Com-mittee on Prevention, Detection. Evaluation, and Treatmentof High Blood Pressure: the JNC 7 report. JAMA 2003;289:2560—72.
[23] Expert Panel on Detection, Evaluation, and Treatment of HighBlood Cholesterol in Adults: Executive Summary of the ThirdReport of the National Cholesterol Education Program (NCEP)Expert Panel on Detection, Evaluation, and Treatment of HighBlood Cholesterol in Adults (Adult Treatment Panel III). JAMA2001;285:2486—97.
[24] Alberti KG, Zimmet P, Shaw J. The metabolic syndrome-a new
worldwide definition. Lancet 2005;366(9491):1059—62.[25] Micha R, Mozaffarian D. Saturated fat and cardiometabolic riskfactors, coronary heart disease, stroke, and diabetes: a freshlook at the evidence. Lipids 2010;45(10):893—905.
[
103
26] Hunter JE, Zhang J, Kris-Etherton PM. Cardiovascular diseaserisk of dietary stearic acid compared with trans, other satu-rated, and unsaturated fatty acids: a systematic review. Am JClin Nutr 2010;91(1):46—63.
27] Siri-Tarino PW, Sun Q, Hu FB, Krauss RM. Saturated fat,carbohydrate, and cardiovascular disease. Am J Clin Nutr2010;91(3):502—9.
28] Swierczynski J, Wołyniec W, Chmielewski M, Rutkowski B.Molecular mechanism of fatty acids impact on plasma lipidprofile (part I). Przegl Lek 2007;64(1):37—41.
29] Clifton PM, Noakes M. Impaired HDL, response to fatin men with coronary artery disease. Atherosclerosis2000;150:159—65.
30] Dreon DM, Fernstrom HA, Campos H, Blanche P, Williams PT,Krauss RM. Change in dietary saturated fat intake is correlatedwith change in mass of large low-density-lipoprotein particlesin men. Am J Clin Nutr 1998;67(5):828—36.
31] Mirmiran P, Ramezankhani A, Azizi F. Combined effects of satu-rated fat and cholesterol intakes on serum lipids: Tehran Lipidand Glucose Study. Nutrition 2009;25:526—31.
32] Baik I, Abbott RD, Curb JD, Shin C. Intake of fish and n-3 fattyacids and future risk of metabolic syndrome. Am Diet Assoc2010;110(7):1018—26.
33] He K, Song Y, Daviglus ML, et al. Accumulated evidence onfish consumption and coronary heart disease mortality: a meta-analysis of cohort studies. Circulation 2004;109:2705—11.
34] Van Tol A, Terpstra AHM, Van den Berg P, Beynen AC. Dietarycorn oil versus olive oil enhances HDL protein turnover andlowers HDL cholesterol levels in hamsters. Atherosclerosis1999;147:87—94.
35] Bos MB, de Vries JH, Feskens EJ, et al. Effect of a high monoun-saturated fatty acids diet and a Mediterranean diet on serumlipids and insulin sensitivity in adults with mild abdominal obe-sity. Nutr Metab Cardiovasc Dis 2010;20(8):591—8.
36] Kelly RB. Diet and exercise in the management of hyperlipi-demia. Am Fam Physician 2010;81(9):1097—102.
37] Petit V, Arnould L, Martin P, et al. Chronic high-fat diet affectsintestinal fat absorption and postprandial triglyceride levels inthe mouse. J Lipid Res 2007;48(2):278—87.
38] Jebb SA, Lovegrove JA, Griffin BA, et al. On behalf of the RISCKStudy Group. Effect of changing the amount and type of fat andcarbohydrate on insulin sensitivity and cardiovascular risk: theRISCK (Reading, Imperial, Surrey, Cambridge, and Kings) trial.Am J Clin Nutr 2010;92(4):748—58.
39] Clifton P, Colquhoun D, Hewat C. Dietary intervention to lowercholesterol. Aust Fam Physician 2009;38(6):424—8.
40] Jenkins DJ, Kendall CW, Marchie A, Faulkner D, Vidgen E, Laps-ley KG, et al. The effect of combining plant sterols, soy protein,viscous fibers, and almonds in treating hypercholesterolemia.
Metabolism 2003;52(11):1478—83.41] Mirmiran P, Noori N, Zavareh MB, Azizi F. Fruit and veg-etable consumption and risk factors for cardiovascular disease.Metabolism 2009;58(4):460—8.



![CPLRE / CONGRESS WHO’S WHO DATABASE MANUEL …€¦ · CPLRE / Congress Who's Who Database Dossier manuel utilisateur MU_CONGRESSDB_FR.doc [Congress Database] Dernière modification](https://img.pdfslide.fr/doc/110x75/5f4c7e82fb63ac754e5792cd/cplre-congress-whoas-who-database-manuel-cplre-congress-whos-who-database.jpg)















![Metabolically healthy obese and metabolic syndrome of the ... · “Western” DP (Odds Ratios [OR] and 95% Confidence Intervals [95% CI]: 1.72, 1.07–2.79 and 1.74, 1.07–2.84,](https://img.pdfslide.fr/doc/110x75/60e1c1c9b944a7043e3358db/metabolically-healthy-obese-and-metabolic-syndrome-of-the-aoewesterna-dp-odds.jpg)








