Embed Size (px)
Citation preview

L'endobrachywsophage : une pathologie fonct ionnel le du tractus digestif sup( rieur
J. STEIN, S. HOEFT, T.R. DeMEESTER University of Southern California School of Medicine, Los Angeles, California (U.S.A.)
Barrett's esophagus: a functional foregut disorder
RI~SUMI~
La pr6sence d'un endobrachy0esophage et de ses complications chez un patient souffrant de reflux gastro-oesophagien r6sulte d'une association de troubles fonctionnels du tractus digestif sup6rieur. Malgr6 une moindre fr6quence du pyrosis et des r6gurgitations acides, les patients porteurs d'un endobrachycesophage, prdsentent un temps d'exposition sup6rieur h un pH inf6rieur h 2, pH inf6rieur ~ 3 et pH inf6rieur h 4, lors des enregistrements par pHm6trie ambulatoire de 24 heures, lorsqu'on tes compare h des patients souffrant d'oesophagite. Ceci r6sulte d'une fr6quence accrue et d'une dur6e prolong6e des 6pisodes de reflux secondaires un~e moindre efficacit6 du sphincter oesophagien inf6rieur, une d6ficience de la clairance 0esophagienne et un accroissement de la s6~r6tion acide basale et apr6s stimulation. L'accentuation d'un reflux duod6no-gastrique chez un patient pr6sentant une d6ficience du sphincter oesophagien inf6rieur est responsable des 6pisodes de reflux alcalin observ6s chez certains patients porteurs d'un endobra- chyoesophage. En cas d'endobrachyoesophage, le reflux alcalin semble pr6disposer aux complications, st6noses et ulc6rations, et paralt avoir un r61e promoteur de la dysplasie et de l'ad6nocarcinome. Ces observations expliquent la fr6quence des 6checs du traitement m6dical chez les patients porteurs d'un endobrachy0esophage et sont en faveur de la correction chirurgicale de l'insuffisance fonctionnelle du sphincter 0esophagien inf6rieur.
SUMMARY
A combination of functional foregut abnormalities are associated with the presence of Barrett's esophagus and its complications in patients with gastroesophageal reflux disease. Despite less hearthburn and regurgitation, patients with Barrett's esophagus have higher % time with pH < 2, pH < 3, and pH < 4 on ambulatory 24-hour esophageal pH monitoring as compared to patients with esophagitis. This is due to an increased frequency and prolonged duration of reflux episodes secondary to a mechanically defective lower esophageal sphincter in combination with compromised esophageal clearance function and increased basal and stimulated gastric acid secretion. Excessive duodenogastric reflux in the presence of a mechanically defective lower esophageal sphincter is responsible for the increased esophageal alkaline exposure observed in some patients with Barrett's esophagus. Alkaline reflux in patients with Barrett's esophagus appears to predispose to the development of complications, i.e. strictures and ulcerations, and may promote dysplasia and the development of adenocarcinoma. These observations explain why medical therapy frequently fails in patients with Barrett's esophagus and support a surgical correction of the defective lower esophageal sphincter.
INTR OD UCTION
L'oesophage recouvert d'6pith61ium cylindrique, c'est-h-dire l'endobrachyoesophage, est actuelle- ment consid6r6 comme une pathologie acquise r6sultant du remplacement de l'6pith61ium 6pider- moide normal par un 6pith61ium cylindrique chez les patients souffrant de reflux gastro-~sophagien [16, 26, 5]. Au moment du diagnostic, environ 50 % des patients porteurs d'un endobrachy0eso- phage pr6sentent d6jh des complications telles que l'0esophagite 6rosive, les st6noses, ulc6rations, la dysplasie et 6ventuellement l'ad6nocarcinome [5]. La diminution de r6sistance du sphincter ~esopha-
gien inf6rieur, la d6ficience de la clairance 0eso- phagienne, la quantit6 et la qualit6 du liquide reflu6, c'est-h-dire l'acidit6 gastrique, pepsine, enzymes pancr6atiques, sels biliaires, peuvent, cha- cun ou ensemble, contribuer ~ la m6taplasie cylin- drique et aux complications des patients souffrant de reflux gastro-oesophagien. Des 6tudes fonction- nelles pr6cises permettant d'appr6cier l'importance relative de ces divers facteurs n'ont 6t6 disponibles que tr6s r6cemment [17, 10, 18]. La pr6sente 6tude passe en revue les anomalies fonctionnelles observ6es en cas d'endobrachyoesophage et leur influence sur la conduite th6rapeutique de ces pa- tients.
Tir6s ~ part : Tom R. DeMEESTER, M.D., University of Southern California School of Medicine, Department of Surgery, 1510 San Pablo Street, Suite 514, Los Angeles, California 90033-4612, (U.S.A.).
Mots-cl& : Complications, endobrachyoesophage, motilit6 oesophagienne, reflux duod6no-gastrique alcalin, s6cr6tion acide.
Key-words : Acid secretion, Barrett's esophagus, complications, duodeno-gastric alcaline reflux, esophageal motility.
Acta Endoscopica Volume 23 - N ~ 2 - 1993 83

Caract~re du reflux gastro-~esophagien
L'exposition de l'ccsophage h l'acide, c'est-~-dire un pH infErieur ~ 2, pH infErieur ~ 3 et pH
infErieur ~ 4, et l'alcalinit6, c'est-~-dire le pH supErieur ~ 7, peuvent 6tre mesurEes de fa~on objective en ambulatoire par pHm6trie de 24 heures. Les details techniques de la pHmEtrie requi6rent une attention particuli~rement impor- tante dans l'investigation des patients porteurs d'un endobrachyoesophage. L'obtention de don- nEes prEcises et reproductibles relatives au reflux alcalin et acide chez ces patients nEcessite l'emploi d'Electrodes de verre stables et la mise en place de I'Electrode de pH ~ 5 cm au-dessus du niveau supErieur du sphincter ~esophagien, dont la posi- tion doit 6tre d~termin~e par manom~trie [17].
Les donnEes de la pHmEtrie oesophagienne mon- trent que la qualitE et ia quantitE du reflux diff6- rent scion que les patients prEsentent ou non une mEtaplasie cylindrique de la muqueuse oesopha- gienne.
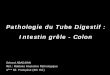
ComparEs ~ des volontaires normaux ou des patients soufrant d'cesophagite, les porteurs d'endobrachyoesophage prEsentent un accroisse- ment important des Episodes cumulEs d'exposition
l'acide ~ diffErents seuils de pH (Fig. 1). Ceci refl6te une augmentation de frEquence et une durEe prolongEe des Episodes de reflux [19, 8]. En outre, les Episodes cumuiEs d'exposition ~ pH alcalin, c'est-~-dire le pourcentage de temps h pH supErieur ~ 7 mesurE par pHmEtrie, est Egalement accru chez les patients avec endobrachy~esophage (Fig. 1). Le temps d'exposition au pH alcalin dEpasse le percentile 95 rEfErE ~ la normale, en particulier chez les patients souffrant de complica- tions de l'endobrachy~esophage, c'est-~-dire les stE- noses, la dysplasie ou les ulcerations (Fig. 2). [1]. Les Etudes d'aspirats de liquide ~esophagien mon-
ao~- ] % du temps total
t f - -~ volontaires normaux
25%. ~ ~esophagite
endobrachy0esophage 20% �9
15% -
10%
5%'
0% pH c 2 pH ( 3 pH( 4 pH) 7
Figure 1
Duree moyenne d'exposition oesophagienne a un pH < 2, pH < 3, pH < 4, et pH > 7 lore d'une pHmetrie oesophagienne de 24 heures chez des volontaires normaux, des patients atteints d'~sophagite et
des malades porteurs d'endobrachy~sophage. �9 : p < 0,01 vs o~sophagite et volontaires normaux
"* : p < 0,05 vs oesophagite et volontaires normaux (d'apres Stein et al., J. Thorac. Cardiovasc. Surg. 1992, avec permission)
Prevalence des patients porteurs d'un end0brachyoesophage
lOO% -
80% "
60%-
40%-
20%"
0%- Nom compliqu~ (N = 18)
[ ~ REFLUX ACIDE
Compliqu~ (N = 23)
l REFLUX ALCALIN
Figure 2
Prevalence d'une exposition et une acidite cesophagienne accrues et un reflux alcalin chez les patients porteurs d'un endobrachycesophage
avec et sans complications. (Modifie d'apres DeMeester et al., Ann. Surg. 1990)
trent des concentrations ElevEes de bile chez les patients dont la muqueuse est anormalement expo- see ~ un pH supErieur h 7 [20]. Cette observation sugg~re que l'exposition accrue ~ un pH supErieur
7 refl~te la presence de liquide biliaire dans ie liquide reflu6, ce qui justifie une attention particu- li6re aux details techniques de I'enregistrement pHmEtrique.
Fonction du sphincter o~sophagien inf6rieur
Chez l'homme, la r6sistance du sphincter oeso- phagien est le premier obstacle au reflux gastro- cesophagien. Cette r6sistance d6pend des effets int6gr6s de la pression ~esophagienne sur toute la longueur du sphinter et de la position de celui-ci, c'est-h-dire la longueur du sphincter expos6e ~ la pression positive intra-abdominale [5, 27].
La manom6trie 0esophagienne montre que ia pression au repos, sur toute la longueur du sphinc- ter, et la longueur de celui-ci en position intra- abdominale sont nettement diminu6es en cas d'endobrachyoesophage par comparaison aux volontaires normaux ainsi qu'aux sujets souffrant d'~esophagite (Fig. 3). Lorsque la manom6trie du sphincter ~esophagien inf6rieur a 6t6 r6alis6e avec des transducteurs de pression h disposition radiale, les pressions sphinct6rielles radiales exerc6es sur toute la longueur du sphincter peuvent sur repr6- sentation graphique, refl6ter un profil tridimen- sionnel des pressions intra-sphinct6riennes. Le volume repr6sent6 par cette figure tridimension- nelle int~gre dans une seule donnEe chiffrEe, les pressions instra-sphinctEriennes et la longueur du sphincter, le vecteur volumEtrique de la pression sphinctErienne, lequel constitue une mesure quan- titative de resistance sphinctErienne au contenu gastrique [21]. Le vecteur volumEtrique de pres- sion sphinctErienne totale ou intra-abdominale est infErieur au percentile 5 de la normale chez plus de 95 % des patients porteurs d'un endobrachy0e- sophage [21].
84 V o l u m e 23 - N ~ 2 - 1993 A c t a E n d o s c o p i c a

16
12
9-
6-
,on ,r snor a x cmfi (Esophagite
mmHg
T
: : :
Presaion
E_~ ~ End~176 e
L0ngueur totale Longueur abd0minale
-2
0 0
Figure 3 Pression moyenne du sphincter cesophagien inferieur, Iongueur abdo- minale et Iongueur totale chez les sujets normaux, des patients avec
cesophagite et porteurs d'endobrachyoesophage. *: p < 0,01 vs oesophagite et volontaires normaux
d'apres Stein et al., J. Thorac. Cardiovasc. Surg. 1992, avec permis- sion)
Fonction de clairance eesophagienne
L'activit6 motrice ~esophagienne constitue un facteur important de la clairance du liquide gastri- que qui a reflu6 dans l'oesophage [5]. L'utilisation combin6e de la radioscopie et de la manom6trie au niveau du corps oesophagien, a permis ~ Kahri- las et al. de montrer r6cemment que la propulsion d'un bolus alimentaire et par cons6quent ia clai- rance du liquide gastrique reflu6, d6pend de contractions p6ristaltiques d'amplitude suffisante. Les contractions non-p6ristaltiques, c'est-~-dire simultan6es, interrompues et isol6es, e t les con- tractions p6ristaltiques d'amplitude insuffisante entralnent un fractionnement du bolus baryt6 et la r6tention du produit de contraste dans le corps
"":~: '.ii'~-~ 1 0111 below UlE8
"iiii, e Cm below UIE8
1~ Cm below UE8
18 crn below UE8
f 1 r-7 Volontaires
(~sophagite I Endobrachy,
~ J
,; ,; .'o .'o ,;o ,~, ,io ,,o ,~o Amplitude (mmHg)
Figure 4
Amplitude moyenne des contractions eesophagiennes apres 10 degluti- tions salivaires, mesur6es respectivement h 1, 6, 11, 16 et 21 cm en dessous du sphincter eesophagien superieur chez des volontaires nor- maux, des patients souffrant d'oesophagite et des malades porteurs
d'endobrachycesophage. ": p < 0.01 vs oesophagite et volontaires normaux.
oesophagien. L'amplitude de contraction minimale n6cessaire a l'occlusion de la lumi6re cesopha- gienne et h la propulsion d'un bolus liquide, est d'environ 300 mmHg [11].
La manom6trie standard du corps ~esophagien chez les patients porteurs d'endobrachy~esophage montre une diminution marqu6e de l'amplitude moyenne des ondes de contraction, en particulier au niveau de la moiti6 inf6rieure de l'oesophage (Fig. 4). L'enregistrement ambulatoire de la moti- lit6 eesophagienne par manom6trie de 24 heures montre que ces anomalies sont parall61es ~ une augmentation de fr6quence des contractions non propulsives et des contractions d'amplitude inf6- rieure ~ 30 mmHg [19, 22]. L'enregistrement com- bin6 pH-manom6trie de 24 heures montre que ces contractions inefficaces entrainent un retard de clairance des diff6rents 6pisodes de reflux, en par- ticulier nocturne, lorsque le sujet est en position dorsale et que la gravit6 ne contribue pas h la clairance du liquide reflu6 [4].
S~cr~tion gastrique acide
L'hypers6cr6tion gastrique peut augmenter I'exposition de la muqueuse oesophagienne l'acide lorsqu'au cours d'6pisodes physiologiques, refluent de grandes quantit6s de liquide tr~s con- centr6 [5]. Chez les patients porteurs d'endobra- chyoesophage (EBO), on constate une augmenta- tion, tant du d6bit basal (BAO) que du d6bit maximal (MAO) (Fig. 5) [19,14]. Selon notre pro- pre exp6rience, l'hypers6cr6tion acide, d6finie sur la base d'un BAO sup6rieur ~ 5 mmol/heure et un MAO sup6rieur ~ 30 mmol/heure, a 6t6 d6mon- tr6e chez environ 40 % des patients atteints d'endobrachycesophage [6]. De m6me, une ten- dance ta des valeurs plus acides s'observe chez les patients porteurs d'endobrachy~esophage lorsqu'ils sont soumis aux variations circadiennes du profil de pH gastrique par 6valuation de pHm6trje gas- trique de 24 heures [19].
30-
2 5
2 0
15"
lO
5
mMol/h
OEsophagite
~ B Endobrachyoasophage
D~bit acide basal Ddbit acide maximal
Figure 5
Valeur moyenne du debit secretoire acide basal (BAO) et apres stimula- tion (MAO) chez des patients souffrant d'eesophagite et des malades
porteurs d'endobrachyeesophage. * : p > 0,01 vs o~sophagite.
A c t a E n d o s c o p i c a V o l u m e 23 - N ~ 2 - 1993 85

Reflux duod6nogastrique
Un reflux duod6nogastrique peut 6tre objectiv6 par technique d'aspiration, h6pato-chol6cysto-scin- tigraphie ou pHm6trie gastrique ambulatoire de 24 heures. Les techniques d'aspiration sont anti- physio|ogiques, inconfortables, et n6cessitent un 6quipement de laboratoire sophistiqu6. Grfice l'h6pato-chol6cysto-scintigraphie, le reflux du contenu biliaire dans l'estomac est identifi6 par l'accroissement de la radioactivit6 dans l'aire gas- trique apr~s injection intra-veineuse d'un d~riv6 de T c 99 iminodiac6tique acide tel que la disofenine (DISIDA). Nous avons montr6 pr6c6demment qu'un syst6me d'6valuation sur base de 16 param6- tres d'enregistrement des variations circadiennes du pH gastrique est sup6rieur h rh6pato-chol6- cysto-scintigraphie dans le diagnostic d'un reflux duod6nogastrique anormal, qu'il est possible d'identifier avec une sensibilit6 de 90 % et une sp6cificit6 de 100 % [23, 7].
La pr6valence d'un reflux duod6nogastrique excessif a 6t6 d6montr6e tant par h6pato-chol6- cysto-scintigraphie clue par pHm6trie gastrique de 24 heures, chez les sujets porteurs d'un endobra- chy~esophage (Fig. 6) [19]. La pr6valence d'un reflux duod6nogastrique major6 est particuli6re- ment marqu6e chez les sujets porteurs de compli- cations de l'endobrachyoesophage, c'est-h-dire st6- noses, dysplasie ou ulc6rations [6, 25, 9].
7~ 1 60% ]
50% -I
40%
Pr(~valence d'un test pathologique Volontaires normaux
(Eosophagite I Endobrachyo~sophage
30*/,
20%
10%
0% H(~pato-chol~cysto-scinUgraphie
0/22
pHm(~trie gastrique de 24 h
Figure 6 Prevalence d'un reflux duodenogastrique excessif demontre par hepato-cholecystographie et pHmetrie gastrique ambulatoire de 24 heures chez des sujets normaux, des patients avec oesophagite et des
malades porteurs d'ehdobrachyoesophage. * : p > 0,01 vs vo]ontaires norrnaux.
Vidange gastrique
Une vidange gastrique retard6e peut 6galement contribuer ~ l'exposition prolong6e de la muqueuse cesophagienne h des contenus gastriques [5]. La vidange gastrique mesur6e par repas isoto- pique constitu6 de farine d'avoine est retard6e ~ la fois chez les patients souffrant d'~esophagite par reflux ou d'endobrachyoesophage [19]. Toutefois,
que les patients soient porteurs ou non d'endobra- chy0esophage, on ne constate pas de diff6rence dans les courbes de vidange gastrique et les mesures du temps de demi-vidange de l'estomac [19].
Les anomalies fonctionnelles et leurs cons6quences sur la conduite th6rapeutique de l'endobrachycesophage
L'investigation fonctionnelle d6taill6e des patients porteurs d'endobrachy~esophage montre que cette affection constitue un stade terminal de la maladie du reflux gastro-0esophagien, caract6ris6 par une exposition ~esophagienne accrue h l'acide, la perte de la r6sistance du sphincter cesophagien inf6rieur, une d6t6rioration de la fonction de clai- rance du corps 0esophagien, et une s6cr6tion acide accrue. Un reflux duod6nogastrique excessif, un temps d'exposition h u n reflux alcalin ont une pr6valence marqu6e chez les sujets porteurs de complications, c'est-h-dire ulc6res, st6noses et dys- plasie. Les anomalies fonctionnelles des patients porteurs d'endobrachycesophage, leur pr6valence et leurs cons6quences sont r6sum6es dans le Tableau 1.
TABLEAU I
PRI~VALENCE ET CONSI~QUENCES DES ANOMALIES FONCTIONNELLES DANS L'ENDOBRACHY(ESOPHAGE
Anomalies Pr6valence Cons6quence
> 90% D6ficience m6canique du sphincter cesopha- gien inf6rieur
Anomalie de la motilit6 du corps 0esophagien :
S6cr6t ion gas t r ique acide accrue :
Reflux duod6nogastri- que excessif :
Sensibilit6 diminu6e :
80 %
40 %
40 %
100 % (9)
Pr6disposition au reflux gastro-oesophagien.
Retard de clairance des 6pisodes de reflux. Dysphagie.
Reflux de liquide gastri- que caustique.
Reflux nocif d'acides biliaires et d'enzymes pancr6atiques.
Absence de sympt6mes d'alarme traduisant une alt6ration muqueuse, faible compliance vis-h- vis du traitement m6- dical.
En cas d'endobrachy~esophage, le temps d'expo- sition accru ~t un liquide gastrique plus concentr6 semble r6sulter d'une perte de la r6sistance du sphincter oesophagien inf6rieur combin6e h une hypers6cr6tion gastrique acide. L'accroissement de la s6cr6tion acide, en pr6sence d'une d6ficience fonctionnelle du sphincter oesophagien peut par cons6quent constituer un facteur de pr6disposition
la m6taplasie cylindrique chez des patients souf- frant de reflux gastro-oesophagien [14].
Dans de telles conditions, une d6ficience de l'activit6 de clairance du corps oesophagien, expose
un allongement de la dur6e du contact avec le
86 V o l u m e 23 - N ~ 2 - 1993 A c t a E n d o s c o p i c a

liquide gastrique reflu6. Ceci se traduit par la dur6e prolong6e des 6pisodes de reflux observ6s chez les patients porteurs d'un endobrachy~eso- phage [18].
Le contr61e du reflux ne tend pas h la r6versibi- lit6 lorsque la paroi 0esophagienne est infiltr6e par une fibrose et que l'amplitude moyenne des contractions s'est abaiss6e en-dessous de 30 mmHg [24]. Ces observations ont deux implica- tions importantes dans le traitement chirurgical. En premier lieu, la perte de la fonction p6ristalti- que de l'endobrachycesophage semble du moins partiellement secondaire ~ des 6pisodes persistants de reflux h travers un sphincter oesophagien ineffi- cace [22]. La d6ficience de la clairance cesopha- gienne allonge h son tour le temps d'exposition de l'0esophage au liquide gastrique et entra~ne la fibrose pari6tale contribuant de cette fa~on ~ ins- taurer un cercle vicieux [22]. Par cons6quent, la correction chirurgicale du trouble fonctionnel sous- jacent, c'est-~-dire la d6fection m6canique du sphincter cesophagien, devrait 6tre recommand6e un stade pr6coce de 1'6volution de la maladie. En second lieu, lorsque la fonction p6ristaltique ceso- phagienne est alt6r6e, une cure anti-reflux doit g~ner mod6r6ment l'6vacuation, et comporter une fundoplicature partielle.
La pr6valence 61ev6e du reflux duod6nogastri- que et du reflux gastro-0esophagien alcalin chez les patients porteurs de complications d'endobrachy- cesophage, montre que la composition du liquide gastrique reflu6 a autant d'importance que les troubles fonctionnels du sphincter dans ie d6velop- pement des st6noses, des ulc~res et de la dyspla- sic. Les 6tudes exp6rimentales montrent qu'un reflux duod6nogastrique alcalin modifie le contenu du liquide gastrique reflu6 et exerce des effets nocifs au niveau de l'eesophage inf6rieur, et pour-
rait constituer un facteur promotionnel du d6ve- Ioppement d'un ad6nocarcinome cesophagien [2, 15]. Pour que le liquide duod6nal alcalin puisse atteindre l'oesophage inf6rieur, il doit traverser i'environnement gastrique acide et vaincre la bar- ri~re de la jonction oeso-gastrique. Seuls des 6pi- sodes de reflux duod6no-gastrique excessif et une fonction sphinct6rienne compromise permettent au liquide duod6nal de refluer sans 6tre neutralis6 dans I'estomac et finalement d'accroitre l'exposi- tion de la muqueuse ~esophagienne aux acides biliaires et aux enzymes pancr6atiques actifs [17, 12]. Ces conditions sont r6unies chez les patients porteurs d'un endobrachy0esophage.
Sans prendre en consid6ration les anomalies physiologiques qui conduisent ~ la m6taplasie cylindrique et ses complications, le traitement m6dical de l'endobrachy~esophage concerne direc- tement la suppression du reflux gastrique acide. Chez les patients souffrant d'une d6ficience du sphincter oesophagien inf6rieur et d'un reflux duo- d6nogastrique excessif, cette approche th6rapeuti- que est sans effet sur le reflux liquide duod6nal. Ceci explique la fr6quence de 1'6chec du traite- ment m6dical chez ies patients porteurs d'endobra- chycesophage, la progression crglniale de la jonc- tion muqueuse oeso-gastrique et l'apparition des st6noses [3].
Par contre, la reconstruction d'une barri6re effi- cace contre le reflux gastro-~esophagien grfice une cure chirurgicale anti-reflux permet plus effi- cacement n'importe quel traitement m6dical, l'abo- lition du reflux de n'importe quel contenu gastri- que, la cicatrisation des ulc6res et des st6noses, l'interruption de la progression de la m6taplasie cylindrique, voire une protection contre la d6g6n6- rescence maligne de l'endobrachyoesophage [6, 13].
RI~FI~RENCES
1. ATTWOOD S.E.A., DeMEESTER T.R., BREMNER C.B., BARLOW A.P., HINDER R.A. - - Alkaline gas- troesophageal reflux: implications in the development of complications in Barrett's columnar-lined lower esophagus. Surgery, 1989, 106, 764-770.
2. A'Iq'WOOD S.E.A., SMYRK T.C., DeMEESTER T.R., MIRVISH S., STEIN H.J., HINDER R.A. - - Duodeno- esophageal reflux and the development of esophageal ade- nocarcinoma in rats. Surgery, 1992, 11, 503-510.
3. BREMNER C.G. - - Barrett's esophagus. Br. J. Surg. 1989, 76, 995-996.
4. BUMM R., FEUSSNER H., EMDE C. - - Interaction of gastroesophageal reflux and esophageal motility in healthy men undergoing combined 24-hour mano/pHmetry. In Lit- tle A.G., FERGUSON M.K., SKINNER D.B. (editors). Diseases of the Esophagus. Futura Publishing Company, Inc., Mount Kisko, NY 1990, 101-113.
5. DeMEESTER T.R., STEIN H.J. - - Gastroesophageal Reflux Disease. In MOODY F.G., JONES R.S., KELLY K.A., NAHRWOLD D.L. and SKINNER D.B. (editors) : ~ Surgical Treatment of Digestive Disease ,~, 2nd edition. Year Book Medical Publishers, Chicago, I l l , 1989, 65-108.
6. DeMEESTER T.R., ATTWOOD S.E.A., SMYRK T.C. et al. - - Surgical therapy in Barrett's esophagus. Ann. Surg., 1990, 212, 528-542.
7. FUCHS K.H., DeMEESTER T.R., HINDER R.A., STEIN H.J., BARLOW A.P. - - Computerized identifica- tion of pathologic duodenogastric reflux. Ann. Surg., 1991, 213, 13-20.
8. GILLEN P., KEELING P., BYRNE P.J., HENNESSY T.P.J. - - Barren's esophagus: pH profile. Br. J. Surg., 1987, 74, 774-776.
9. GILLEN P., BYRNE P.J., HEALLY M., O 'MOORE R.R., HENNESSY T.P.J. - - Implication of duodenogastric reflux in the pathogenesis of Barrett's esophagus. Br. J. Surg., 1988, 75, 540-543.
10. IASCONE C., DeMEESTER T.R., LIT]'LE A.G., SKIN- NER D.B. - - Barrett's esophagus : functional assessment, proposed pathogenesis and surgical therapy. Arch. Surg., 1983, 118, 543-549.
11. KAHRILAS P.J., DODDS W.J., HOGAN W.J. - - Effect of peristaltic dysfunction on esophageal volume clearance. Gastroenterology, 1988, 94, 73-80.
Acta Endoscopica Volume 23 - N ~ 2 - 1993 87

12. Lin K.M., UEDA R.K., HINDER R.A., STEIN H.J., DeMEESTER T . R . - - The etiology and importance of alkaline esophageal reflux. Am. J. Surg., 1991, 162, 553- 557.
13. McCallum R.W., POLEPALLE S., DAVENPORT K., BOYD S . - - Role of antireflux surgery against dysplasia in Barrett's esophagus. Gastroenterology, 1991, 100, A121.
14. MULHOLLAND M.W., REID, LEVINE D.S., RUBIN C.E. - - Elevated gastric acid secretion in patients with Barrett's metaplastic epithelium. Dig. Dis. Sci., 1989, 34, 1329-1335.
15. PERA M., CARDESA A., BOMBI J .A. et al. -- Influence of esophagoduodenostomy on the induction of adenocarcinoma of the distal esophagus in Sprague-Dawley rats by subcutaneous injection of 2,6 dimethynitrosomor- pholine. Cancer Research, 1989, 49, 6803-6808.
1 6 . S P E C H L E R S . J . , G O Y A L R R . K . - - Barrett's esophagus. N. Engl. J. Med., 1986, 315, 362-371.
17. STEIN H.J., BARLOW A.P., DeMEESTER T.R., HIN- DER R . A . - - Complications of gastroesophageal reflux disease : role of the lower esophageal sphincter, esophageal acid/alkaline exposure, and duodenogastric reflux. Ann. Surg., 1992, 216, 35-43.
18. STEIN H.J., HOEFT S., DeMEESTER T.R. - - Reflux and motility pattern in Barrett's esophagus. Dis. Esoph., 1992, 5, 21-28.
19. STEIN H.J., HOEFT S., DeMEESTER T.R. - - Functio- nal foregut abnormalities in Barrett's esophagus. J. Thorac. Cardiovasc. Surg., 1992 (in press).
20. STEIN H.J., FEUSSNER H., BARTHLEN W., DeMEESTER T . R . , S I E W E R T J . R . - - Alkalischer Gas- tro6sophagealer Reflux - Quantifizering und klinishe Rele- vanz. Langenbecks Arch. Chit. For., 1992, 87-91.
21. STEIN H.J., DeMEESTER T.R., NASPETI'I R., JAMIE- SON J., PERRY R. - - The three-dimensional lower eso- phageal sphincter pressure profile in gastroesophageal re- flux disease. Ann. Surg., 1991, 214, 374-384.
22. STEIN H.J., EYPASCH E.P., DeMEESTER T.R. - - Cir- cadian esophageal motor function in patients with gastroe- sophageal reflux disease. Surgery, 1990, 108, 769-777.
23. STEIN H.J., HINDER R.A., DeMEESTER T.R., LLOYD B.A., FUCHS K.F. - - Clinical use of 24-hour gastric pH monitoring versus DISIDA scanning in the diagnosis of pathologic duodenogastric reflux. Arch. Surg., 1990, 125, 966-971.
24. STEIN H.J., BREMNER R.M., JAMIESON J., DeMEESTER T . R . - - Effect of Nissen fundoplication on esophageal motor function. Arch. Surg., 1992, 127, 788- 792.
25. WARING J.P., LEGRAND J., CHIBICHIAN A., SANOWSKI R . A . - - Duodenogastric reflux in patients with Barrett's esophagus. Dig. Dis. Sci., 1990, 35, 759-762.
26. WINTERS C., SPURLING T.J., CHOBANIAN S.J. et aL - - Barrett's esophagus : a prevalent, occult complication of gastroesophageal reflux disease. Gastroenterology, 1987, 92, 118-124.
27. ZANINOT]?O G., DeMEESTER T.R., SCHWlTZER W., JOHANSSON K.E., CHENG S.C. - - The lower esopha- geal sphincter in health and disease. Am. J. Surg., 1988, 155, 104-109.
I N T R O D U C T I O N
Columnar lined esophagus, i. e. Barrett's esopha- gus, is today commonly regarded as an acquired condition resulting from replacement of the normal squamous esophageal epithelium by columnar epithelium in patients with gastroesophageal reflux disease [16, 26, 5]. At the time of diagnosis about 50 % of patients with Barrett's esophagus already present with complications such as erosive esophagitis, strictures, ulcerations, dysplasia, or even adenocarcinoma [5]. Decreased lower esophageal sphincter resistance, compromised esophageal clearance function, and the quantity and quality of the refluxate, i. e. gastric acid, pepsin, pancreatic, enzymes, and bile acids, may indivi- dually or in combination contribute to columnar metaplasia and its complications in patients with gastroesophageal reflux. Detailed functional studies to assess the relative importance of these factors have, however, only recently become available [17, 10, 18]. The functional abnormalities in patients with Barrett's esophagus and their effect on the management of patients with the disorder are reviewed.
R e f l u x P a t t e r n
Esophageal exposure to adic, i. e. pH < 2, pH < 3, and pH < 4, and alkalinity, i. e. pH > 7, can be measured objectively by ambulatory 24-hour esophageal pH monitoring. Attention to technical details of pH monitoring is, however, particularly
important when evaluating patients with Barrett's esophagus. In order to obtain accurate and repro- ductible data on acid and alkaline reflux in patients with Barrett's esophagus it is essential that only stable glass electrodes are used and that the pH electrode is placed 5 cm above the upper border of the m a n o m e t r i c a l l y d e t e r m i n e d lower esophageal sphincter [17].
Esophageal pH monitoring shows that the quality and quantity of the refluxate is different in reflux patients with and without Barrett's columnar meta- plasia. Compared to normal volunteers and patients with esophagitis, patients with Barett's esophagus have a markedly increased cumulative esophageal exposure to acid at various pH thresholds (Figure 1). This is due to an increased frequency and prolonged duration of reflux episode [19, 8]. In addition the cumulative esophageal exposure to alkalinity, i. e. the % time with pH > 7 on esophageal pH monitoring, is also increased in patients with Barrett's esophagus (Figure 1). Esophageal alkaline exposure exceeds the 95th per- centile of normal particularly in those patients who have complications of Barrett's esophagus, i. e. a stricture, dysplasia, or ulcerations (Figure2)[1]. Esophageal aspiration studies have shown high con- centrations of bile in aspirate from patients with abnormally high esophageal exposure to pH > 7 [20]. This would suggest that increased esophageal exposure to pH > 7 reflects the presence of duodenal juice in the refluxate provided that
88 Volume 23 - N ~ 2 - 1993 Acta Endoscopica

25%'
20%
% Total Time
Normal Volunteers
I ~ Eaophagltl8
I Barrett'a Esophagus
15%
10%
5%
0 % . . . . . .
pH (2 p H ( 3 p H ( 4 p H ) 7
Figure 1
Mean esophageal exposure time to pH < 2, pH < 3 , pH < 4, and pH > 7 on 24-hour esophageal pH monitoring in normal volunteers,
patients with esophagitis, and patients with Barrett's esophagus. *: p < 0.01 vs esophagitis and normal volunteers. **: p < 0.05 vs esophagitis and normal volunteers.
(From Stein et aL, J. Thorac. Cardiovasc. Surg., 1992, with permission).
Prevalence in Patients with Barrett'l
100% -
80% -
60%
40%
20%
0% Uncomplicated (No18)
/ Complicated (N-23)
[ ~ ACID REFLUX 1 ALKALINE REFLUX
Figure 2
Prevalence of increased esophageal acid and alkaline exposure in patients with Barrett's esophagus with and without complications.
(Modified from DeMeester et aL, Ann. Surg., 1990).
assiduous attention is paid to the technical details of the esophageal pH recording.
Lower Esophageal Sphincter Function
The primary barrier against gastroesophageal reflux in man is the resistance of the lower esophageal sphincter. This resistance depends on the integrated effects of sphincter pressures exerted over the entire length of the sphincter and the position of the sphincter, i. e. the length of sphinc- ter exposed to the positive pressure environment of the abdomen [5, 27].
Esophageal manometry shows that resting pressure, overall length, and abdominal length of the lower esophageal sphincter are markedly decreased in patients with Barrett's esophagus as compared to patients with esophagitis or normal volunteers (Figure3). When manometry of the
15
12
6-
3
mmHg
T ~ Normal Volunteers
: ~ Esophagltla
i l l Barrett'e Esophagus
cmfi
Pressure
T
I Overall Length
i Abdominal Length
-2
0 -- 0
Figure 3
Mean lower esophageal sphincter pressure, abdominal length, and overall length in normal volunteers, patients with esophagitis and
patients with Barrett's esophagus. *: p < 0.01 vs esophagitis and normal volunteers.
(From Stein et aL, J. Thorac. Cardiovasc. Surg., 1992, with permission).
lower esophageal sphincter is performed with radially oriented pressure transducers, radial sphincter pressures exerted over the entire length of the sphincter can be shown graphically as a three dimensional sphincter pressure profile. The volume circumscribed by this three dimensional figure integrates sphincter pressure and length into one number, the sphincter pressure vector volume, which is a quantitative measure of sphincter resis- tance to gastric contents [21]. The total or intrab- dominal sphincter pressure vector volume is below the 5th percentile of normal in over 95 % of patients with Barrett's esophagus [21].
Esophageal Clearance Function
Esophageal motor activity is an important factor in the clearance of refluxed gastric contents [5]. Using simultaneous fluoroscopy and manometry of the esophageal body Kahrilas et al. have recently shown that propulsion of a bolus and consequently clearance of refluxed gastric contents depends on peristaltic contractions of sufficient amplitude. Non- peristaltic contractions, i.e. simultaneous, inter- rupted and isolated contractions, and peristaltic contractions of insufficient amplitude result in split- ting of the barium bolus and retention of contrast medium in the esophageal body. The minimal con- traction amplitude required to occlude the esophageal lumen and propel a liquid bolus is about 30 mmHg [11].
Standard manometry of the esophageal body in patients with Barrett's esophagus shows a markedly decreased mean amplitude of contractions particu- larly in the distal half of the esophagus (Figure 4). This is paralleled by an increased frequency of non-propulsive contractions and contractions with an amplitude below 30 mmHg on ambulatory 24- hour esophageal motility monitoring [19, 22]. Com- bined esophageal manometry and pH monitoring shows that these ineffective contractions result in a delayed clearance of reflux episodes particularly
A c t a E n d o s c o p i c a V o l u m e 23 - N ~ 2 - 1993 89

(
[ ~ Elophligltlll I B&rrett'l
~"~'s 20 40 60 80 100 120 140 leO 180 ,l~nplltude {mmHg)
Figure 4
Mean of amplitude of esophageal contractions following 10 wet swal- lows measured 1, 6, 11, 16, and 21 cm below the upper esophageal sphincter in normal volunteers, patients with esophagitis and patients with Barrett's esophagus,
*: p < 0.01 vs esophagitis and normal volunteers.
during the night when the subject is in the supine position and gravity does not aid in clearance of the refluxate [4].
Gastric Acid Secretion
Gastric acid hypersecretion can increase esophageal acid exposure by the physiologic reflux of large quantities of highly concentrated gastric acid [5].
Both basal acid output (BAO) and maximum acid output (MAO) are increased in patients with Barrett's esophagus (Figure5) [19, 14]. In our experience, gastric acid hypersecretion, defined as BAO above 5 mmol/hour and MAO above 30 mmol/hour, can be documented in about 40 %
3 0 -
2 5
20
15
1 0
5
mMol/h
Eaophagltla
I Barrett'e Esophagus
t~
-7-
Basal Acid Output Maximum Acid Output
Figure 5
Mean basal (BAO) and stimulated (MAO) gastric acid secretion in patients with esophagitis and patients with Barrett's esophagus.
* : p < 0.01 vs esophagitis.
of patients with Barrett's esophagus [6]. Similarly, a shift towards more acidic values can be observed in patients with Barrett's esophagus when their circa- dian gastric pH profile is evaluated by 24-hour gastric pH monitoring [19].
Duodenogastric Reflux
Duodenogastric reflux can be objectively assessed by aspiration techniques, cholescintigraphy, or ambulatory 24-hour gastric pH monitoring. Aspira- tion techniques are unphysiologic, cumbersome, and require a sophisticated laboratory. With choles- cintigraphy, reflux of duodenal content into the stomach is recognized by the increase of radioacti- vity in the area of the stomach after the intravenous injection of Tc 99m iminodiacetic acid derivates such as disofenin (DISIDA). We have previously shown that a scoring system based on 16 parameters of the circadian gastric pH record is superior to cholescin- tigraphy in the diagnosis of excessive duodenogas- tric reflux and can detect the condition with a sensitivity of 90 % and specificity of 100 % [23, 7].
Both, cholescintigraphy and gastric pH monito- ring show an increased prevalence of excessive duodenogastric reflux in patients with Barrett's esophagus (Figure 6) [19]. Excessive duodenogastric reflux is particularly prevalent in patients with com- plications of Barrett's esophagus, i. e. stricture, dysplasia, or ulcerations [6, 25, 9}.
7 0 % -~ Prevalence of /
6 0 % t a Pathologlc Test
| 50% 1
4 0 %
Normal Volunteers
Eaophsglt la
1 Barrett*s Esophagus
t
3 0 %
2 0 %
10'/.
0% C h o l e s c i n t i g r a p h y
0/22
G a s t r i c p H - M o n i t o r i n g
Figure 6
Prevalence of excessive duodenogastric reflux on cholescintigraphy and 24-hour ambulatory gastric pH monitoring in normal volunteers,
patients with esophagitis, and patients with Barrett's esophagus. * : p < 0.01 vs normal volunteers.
Gastric Emptying
Delayed gastric emptying may also contribute to increased esophageal exposure to gastric contents [5]. Gasiric emptying of a radiolabeled oatmeal is delayed in both reflux patients with esophagitis and those with Barrett's esophagus [19]. There is, how- ever, no difference in the gastric emptying curves and gastric half emptying time between reflux patients with or without Barrett's esophagus [19].
90 Volume 23 - N ~ 2 - 1993 Acta Endoscopica

Functional Abnormalit ies and Their Consequences for the Management of Barrett's Esophagus
Detailed evaluation of foregut function in patients with Barrett's esophagus shows that the condition represents end stage reflux disease which is charac- terized by a markedly increased esophageal expo- sure to acid, the loss of lower esophageal sphincter resistance, deteriorated clearance function o f the esophageal body, and increased gastric acid secre- tion. Excessive duodenogastric reflux and increased esophageal alkaline exposure are particularly preva- lent in patients with complications i. e. ulceration, stricture, and dysplasia. The functional abnor- malities in patients with Barrett's esophagus, their prevalence, and the consequences are summarized in table 1.
TABLE I FUNCTIONAL ABNORMALITIES, THEIR PREVALENCE
AND CONSEQUENCES IN BARRETP'S ESOPHAGUS
Abnormality Prevalence Consequence
> 90% !Mechanically defective lower esophageal sphin- cter : Abnormal motor function of the tubular esophagus : Increased gastric acid secretion : Excessive duodenogas- tric reflux :
Decreased sensitivity :
80 %
40 %
40 %
tOO % (?)
Predisposes to free reflux.
Delayed clearance of reflux episodes. Dysphagia. Reflux of caustic gastric juice. Reflux of noxious bile acids and pancreatic enzymes. No symptoms as war- ning signs for mucosal injury, poor compliance with medical therapy.
The increased esophageal exposure time to con- centrated gastric acid in Barrett's esophagus appears to be due to a loss of lower esophageal sphincter resistance in combination with gastric acid hyperse- cretion. Increased gastric acid secretion in the pre- sence of a mechanically defective lower esophageal sphincter may therefore represent a predisposing condition for columnar cell metaplasia in patients with gastroesophageal reflux disease [14].
The compromised clearance activity of the esophageal body in this situation further prolongs esophageal exposure to refluxed gastric juice. This is reflected in the prolonged duration of reflux episodes in patients with Barrett's esophagus [18]. Reflux control does not lead to recovery of esophageal contractility once fibrosis of the esophageal wall has developed and the mean amplitude of contractions has deteriorated below
3 0 m m H g [24]. These observations have two important implications regarding surgical therapy. First, the loss of peristaltic function in Barrett's esophagus appears to be at least in part secondary to persistent reflux across a mechanically defective lower esophageal sphincter [22]. Compromised clearance in turn prolongs esophageal exposure to gastric juice and causes fibrosis of the esophageal wall initiating a vicious cycle [22]. Consequently, the surgical correction of the underlying defect, i. e. the mechanically defective lower esophageal sphinc- ter, should be encouraged early in the course of the disease. Second, once esophageal peristalsis has deteriorated, an antireflux repair with little outflow obstruction, i. e. a partial fundoplication, should be considered.
The high prevalence of excessive duodenogastric and alkaline gastroesophageal reflux in patients with complications of Barrett's esophagus indicates that the composition of refluxed gastric juice is as important as a mechanically defective sphincter in the development of strictures, ulcers, and dysplasia. Experimental studies show that alkaline duodenogastric reflux modifies the content and injurious effects of refluxed gastric juice in the distal esophagus and may promote the development of esophageal adenocarcinoma [2, 15].
In order for alkaline duodenal juice to reach the distal esophagus it has to cross the acidic gastric environment and the barriers at the gas- troesophageal junction. Only in situations of exces- sive duodenogastric reflux and compromised lower esophageal sphincter resistance, will refluxed duodenal juice not be neutralized in the stomach and can result in an increased esophageal exposure active bile acids and pancreatic enzymes [17, 12]. These conditions are given in patients with Barrett's esophagus.
Regardless of the underlying physiologic abnor- mality leading to columnar cell metaplasia and its complications the current medical therapy is aimed only at suppressing acid gastroesophageal reflux. In patients with a mechanically defective lower esophageal sphincter and excessive duodenogastric reflux this approach allows the unabated reflux of duodenal juice. This may explain why in patients with Barrett's esophagus medical therapy fails and may even allow the upward progression of the squamocolumnar junction and the development o f structures [3]. In contrast, reconstruction of an effective barrier at the gastroesophageal junction by a surgical antireflux procedure can effectively abo- lish reflux of any gastric content, heal ulcerations and strictures, halt the progression of columnar epithelium, and may even provide more effective protection against malignant degeneration of the columnar epithelium than medical management [6, 13].
Acta Endoscopica Volume 23 - N ~ 2 - 1993 91