Embed Size (px)
Citation preview
443
1. Lahaye D, en D Bisschop A. Preventieve gezondheidszorgen ter voorkoming vanberoepsziekten. Cah Arbeidsgeneesk 1984; XXI: 133-36.
2. Jacques P. Sero-epidemiologie van hepatitis B bij 20 000 werknemers van de
gezondheidssector. Licentiaatsthesis: Leuven, 1983.3. Institut National de Recherche et de Sécurité. Statistiques des accidents du travail et
des maladies professionnelles. Travail et sécurité, Paris, 1981-1985.4. Maruna H, Winter N. Die Hepatitis-B-Impfaktion der sozialen
Unfallversicherungstrager fur die Berufe in Gesundheits- und Fürsorgewesen derRepublik Österreich. Z Unfallchir Vers Med Berufskr 1986; 79: 217-26.
Environmental Health
The final session of the United Nations Vienna Convention for theProtection of the Ozone layer is to be held in Montreal in the secondweek of September.
OZONE DEPLETION AND CANCER RISK
ROBIN RUSSELL JONES
St John’s Hospital for Diseases of the Skin, London WC2H 7BJ
THE absorption of ultraviolet radiation by stratosphericozone (03) is crucial to the protection of living organisms.About 3% of the sun’s electromagnetic output is emitted asUV radiation, but only a fraction reaches the surface of theearth. UVC in the 240-290 nm range is virtually eliminatedby ozone, and only a proportion of UVB (290-320 nm)penetrates the terrestrial environment. Because UVB andUVC span the photo absorption spectrum of DNA, ozone iscrucial to the viability of primitive life forms, particularly inaquatic ecosystems, and in human beings it greatly limits thecarcinogenic impact of solar radiation. Plant photosynthesis,too, is intimately linked to ambient levels of0, 03, and solarradiation. 1,2
It is over ten years since the scientific community wasawakened to the possibility that man-made chemicals mightdamage the ozone layer.3 The chemical compounds knownas chlorofluorocarbons (CFCs) were identified as being ofparticular concern owing to their prolonged residence timein the atmosphere. Only in the United States was this theorytaken seriously by regulatory bodies; CFCs were banned asaerosol propellants. CFC production has continued toincrease worldwide, and atmospheric levels are growing at arate of 5% per annum. Public concern has risen also-first,because serious ozone depletion is predicted in the nearfuture; second, because there is an increased awarenessabout the health effects of UV irradiation. In the UK, thishas been highlighted most recently by the report from theRoyal College of Physicians on the relation between UVexposure and skin cancer.
4
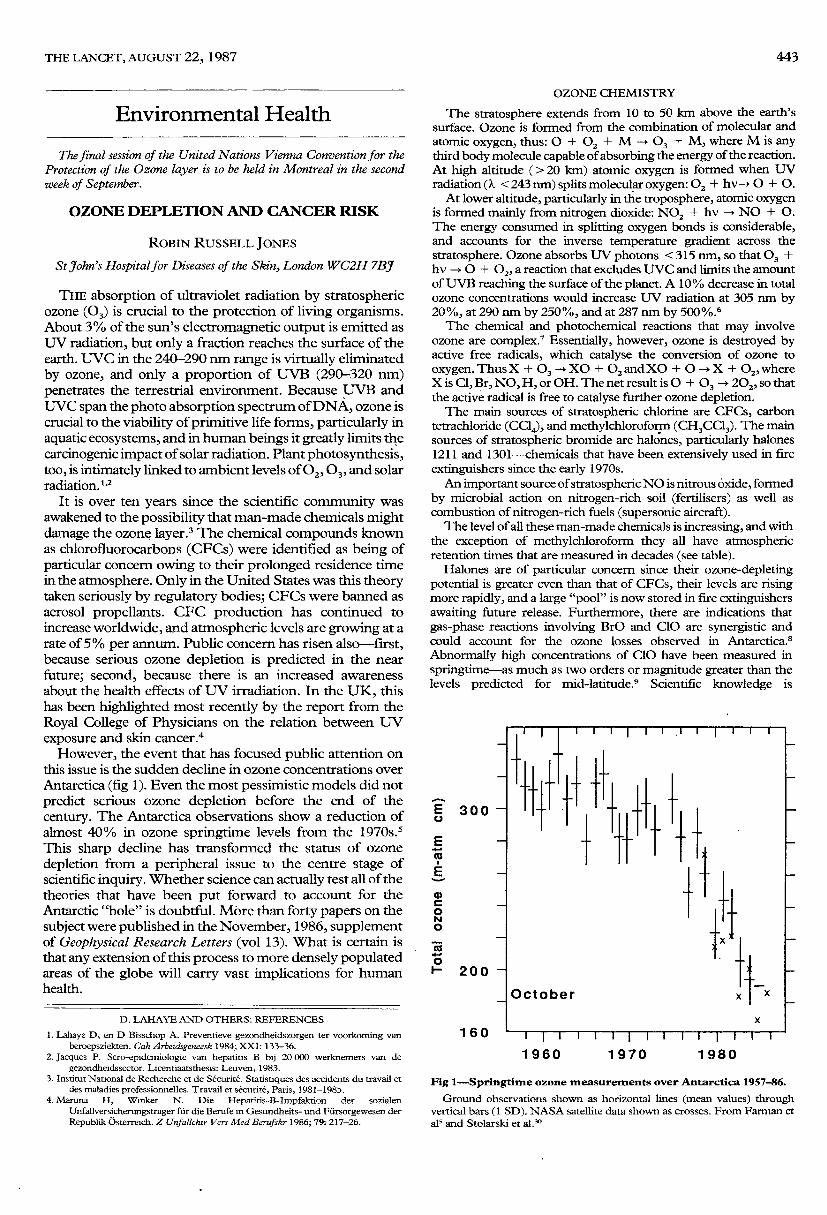
However, the event that has focused public attention onthis issue is the sudden decline in ozone concentrations overAntarctica (fig 1). Even the most pessimistic models did notpredict serious ozone depletion before the end of thecentury. The Antarctica observations show a reduction ofalmost 40% in ozone springtime levels from the 1970s.5This sharp decline has transformed the status of ozonedepletion from a peripheral issue to the centre stage ofscientific inquiry. Whether science can actually test all of thetheories that have been put forward to account for theAntarctic "hole" is doubtful. More than forty papers on thesubject were published in the November, 1986, supplementof Geophysical Research Letters (vol 13). What is certain isthat any extension of this process to more densely populatedareas of the globe will carry vast implications for humanhealth.
OZONE CHEMISTRY
The stratosphere extends from 10 to 50 km above the earth’ssurface. Ozone is formed from the combination of molecular andatomic oxygen, thus: 0 + O2 + M - 03 + M, where M is anythird body molecule capable of absorbing the energy of the reaction.At high altitude (> 20 km) atomic oxygen is formed when UVradiation (k < 243 nm) splits molecular oxygen: O2 + hv-> 0 + 0.At lower altitude, particularly in the troposphere, atomic oxygen
is formed mainly from nitrogen dioxide: N02 + hv — NO + 0.The energy consumed in splitting oxygen bonds is considerable,and accounts for the inverse temperature gradient across thestratosphere. Ozone absorbs LTV photons < 315 nm, so that 03 +hv — 0 + O2, a reaction that excludes UVC and limits the amountofUVB reaching the surface of the planet. A 10% decrease in totalozone concentrations would increase UV radiation at 305 nm by20%, at 290 nm by 250%, and at 287 nm by 500%.6The chemical and photochemical reactions that may involve
ozone are complex.7 Essentially, however, ozone is destroyed byactive free radicals, which catalyse the conversion of ozone tooxygen. Thus X + 0, --* XO + 02andXO + 0 -j X + 02,whereX is Cl, Br, NO, H, or OH. The net result is 0 + 03 - 202, so thatthe active radical is free to catalyse further ozone depletion.The main sources of stratospheric chlorine are CFCs, carbon
tetrachloride (CCI4), and methylchloroform (CH3CCI3). The mainsources of stratospheric bromide are halones, particularly halones1211 and 1301-chemicals that have been extensively used in fireextinguishers since the early 1970s.An important source of stratospheric NO is nitrous oxide, formed
by microbial action on nitrogen-rich soil (fertilisers) as well ascombustion of nitrogen-rich fuels (supersonic aircraft).The level of all these man-made chemicals is increasing, and with
the exception of methylchloroform they all have atmosphericretention times that are measured in decades (see table).
Halones are of particular concern since their ozone-depletingpotential is greater even than that of CFCs, their levels are risingmore rapidly, and a large "pool" is now stored in fire extinguishersawaiting future release. Furthermore, there are indications thatgas-phase reactions involving BrO and C10 are synergistic andcould account for the ozone losses observed in Antarctica.8
Abnormally high concentrations of C10 have been measured inspringtime-as much as two orders or magnitude greater than thelevels predicted for mid-latitude.9 Scientific knowledge is
Fig I-Springtime ozone measurements over Antarctica 1957-86.
Ground observations shown as horizontal lines (mean values) throughvertical bars (1 SD). NASA satellite data shown as crosses. From Farman etals and Stolarski et all
444
ANNUAL INCREASES AND ATMOSPHERIC RETENTION TIMES
incomplete, but man-made chemicals are clearly implicated as oneof the prime reasons for the observed changes in stratospheric ozonein the southern hemisphere.
BIOLOGICAL CONSEQUENCES
UV exposure is closely linked to the aetiology ofmelanoma and non-melanomatous skin cancer. In caucasian
populations, chronic UV exposure seems to be the majordeterminant of basal-cell carcinoma and squamous-cellcarcinoma. Thus, both tumours occur predominantly onlight-exposed areas, their frequency increases with age, andthey are most frequent in fair-skinned people who sunburneasily and in those who spend time outdoors.lO An increasedrate of both tumours is seen in xeroderma pigmentosum, anautosomal recessive genodermatosis characterised bypremature ageing of the skin and specific repair defects ofUV-induced DNA damage." Finally, there is an inverserelation with latitude-somewhat stronger for squamous-cell than for basal-cell carcinoma.1oThe relation between UV exposure and cutaneous
melanoma is more complex. Of the four clinicopathologicaltypes, only lentigo maligna melanoma seems to relate tocumulative UV exposure. Thus lesions arise on light-exposed areas in elderly individuals, and are associatedhistologically with solar elastosis.12 By contrast, acral
lentiginous melanoma, superficial spreading melanoma, andnodular malignant melanoma occur in younger age groups,and are not confined to chronically sun-damaged areas ofskin. Even so, a relation between melanoma and UV
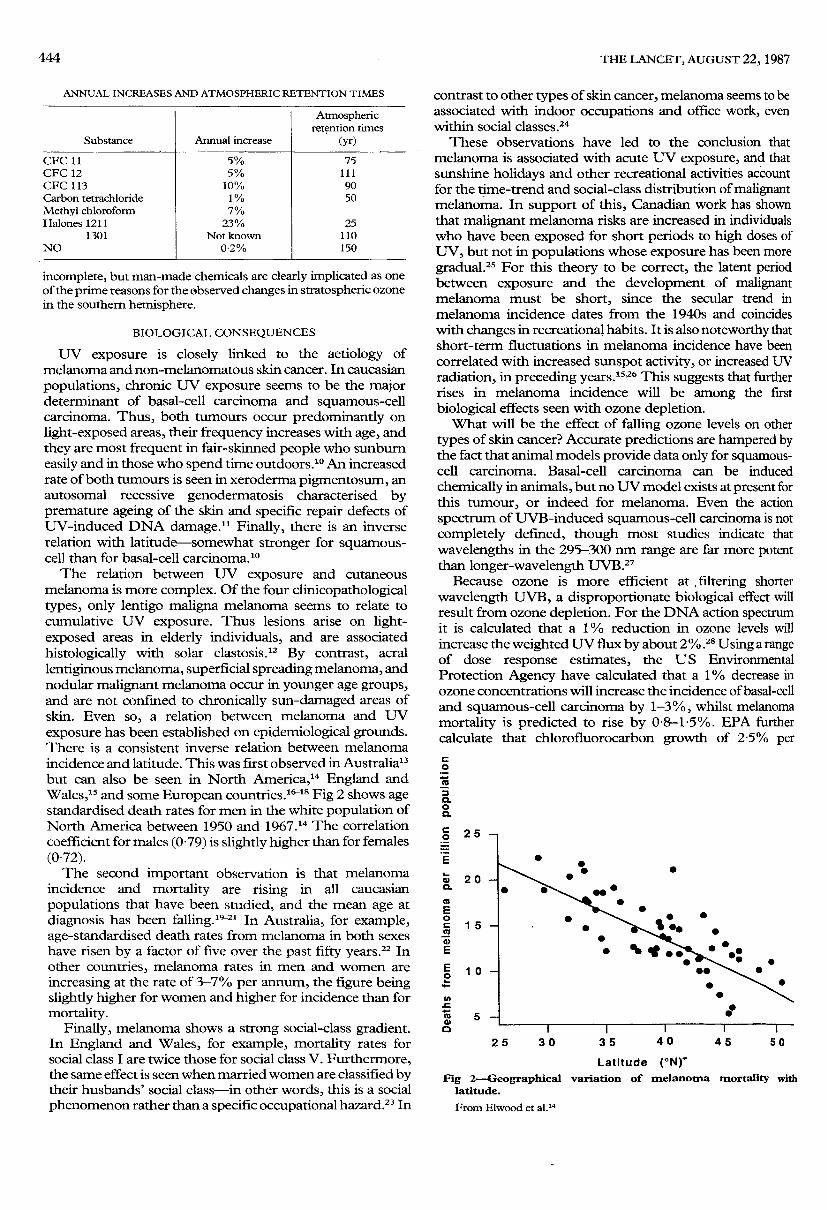
exposure has been established on epidemiological grounds.There is a consistent inverse relation between melanomaincidence and latitude. This was first observed in Australia13but can also be seen in North America,14 England andWales,15 and some European countries.16-18 Fig 2 shows agestandardised death rates for men in the white population ofNorth America between 1950 and 1967.14 The correlationcoefficient for males (0-79) is slightly higher than for females(0-72).The second important observation is that melanoma
incidence and mortality are rising in all caucasian
populations that have been studied, and the mean age atdiagnosis has been falling.19-21 In Australia, for example,age-standardised death rates from melanoma in both sexeshave risen by a factor of five over the past fifty years.22 Inother countries, melanoma rates in men and women areincreasing at the rate of 3-7% per annum, the figure beingslightly higher for women and higher for incidence than formortality.
Finally, melanoma shows a strong social-class gradient.In England and Wales, for example, mortality rates forsocial class I are twice those for social class V. Furthermore,the same effect is seen when married women are classified bytheir husbands’ social class-in other words, this is a socialphenomenon rather than a specific occupational hazard.23 In
contrast to other types of skin cancer, melanoma seems to beassociated with indoor occupations and office work, evenwithin social classes.24
These observations have led to the conclusion thatmelanoma is associated with acute UV exposure, and thatsunshine holidays and other recreational activities accountfor the time-trend and social-class distribution of malignantmelanoma. In support of this, Canadian work has shownthat malignant melanoma risks are increased in individualswho have been exposed for short periods to high doses ofUV, but not in populations whose exposure has been moregradual .25 For this theory to be correct, the latent periodbetween exposure and the development of malignantmelanoma must be short, since the secular trend inmelanoma incidence dates from the 1940s and coincideswith changes in recreational habits. It is also noteworthy thatshort-term fluctuations in melanoma incidence have beencorrelated with increased sunspot activity, or increased UVradiation, in preceding years. 1526 This suggests that furtherrises in melanoma incidence will be among the first
biological effects seen with ozone depletion.What will be the effect of falling ozone levels on other
types of skin cancer? Accurate predictions are hampered bythe fact that animal models provide data only for squamous-cell carcinoma. Basal-cell carcinoma can be induced
chemically in animals, but no UV model exists at present forthis tumour, or indeed for melanoma. Even the action
spectrum of UVB-induced squamous-cell carcinoma is notcompletely defined, though most studies indicate that
wavelengths in the 295-300 nm range are far more potentthan longer-wavelength UVB.27
Because ozone is more efficient at filtering shorter
wavelength UVB, a disproportionate biological effect willresult from ozone depletion. For the DNA action spectrumit is calculated that a 1 % reduction in ozone levels willincrease the weighted UV flux by about 2% . Using a rangeof dose response estimates, the US EnvironmentalProtection Agency have calculated that a 1 % decrease inozone concentrations will increase the incidence of basal-celland squamous-cell carcinoma by 1-3%, whilst melanomamortality is predicted to rise by 0-8-15%. EPA furthercalculate that chlorofluorocarbon growth of 25% per
Fig 2-Geographical variation of melanoma mortality withlatitude.
From Elwood et aU4
445
Fig 3--Projected ozone depletion at different latitudes up to 2030.
From Isaksen.31
annum will cause an additional one million skin cancers, and20 000 deaths over the lifetime of the existing USpopulation. Whilst these figures must be regarded as
tentative, they do provide a perspective on the magnitude ofthe health issues.The impact on environment and climate is more difficult
to predict. Major changes in total column ozone will disturbphotosynthesis and reduce crop yield for many species ofcultivar. Aquatic organisms, particularly phytoplankton,zooplankton, and the larval stages of certain fish, are
sensitive to small increments in UV exposure. It has beencalculated that a 10% reduction in total column ozone willrequire a migration of more than 30° of latitude to restoreequilibrium. The effects on the aquatic food chain, fishproduction, and oxygen output from the ocean could dwarfthe risks to human health.
THE FUTURE
Computer modelling of ozone depletion needs to takeaccount of the hundreds of chemical and photochemicalreactions that take place in the stratosphere, and ofcompensating effects at lower altitude. As ozone levels in theupper stratosphere decline, increased penetration of UVBaccelerates ozone production in the lower stratosphere andtroposphere. This "self-healing" effect diminishes with
increasing latitude, and disappears beyond 40° latitude. Atmid-latitude ozone depletion in the upper stratosphere isexpected to be offset by ozone accumulation in the
troposphere so that total column ozone will remain more orless constant. Data from a global network of groundmonitoring stations are consistent with this hypothesis,28though unpublished NASA satellite data indicate that ozonedepletion in the upper stratosphere is considerably moreadvanced than predicted by the two-dimensional models.29At extreme latitudes the Nimbus 7 data have confirmed the
presence of severe ozone depletion over Antarctica30 andhave provided evidence of a more recent decline over theNorth Pole.Some chemicals, particularly carbon dioxide and
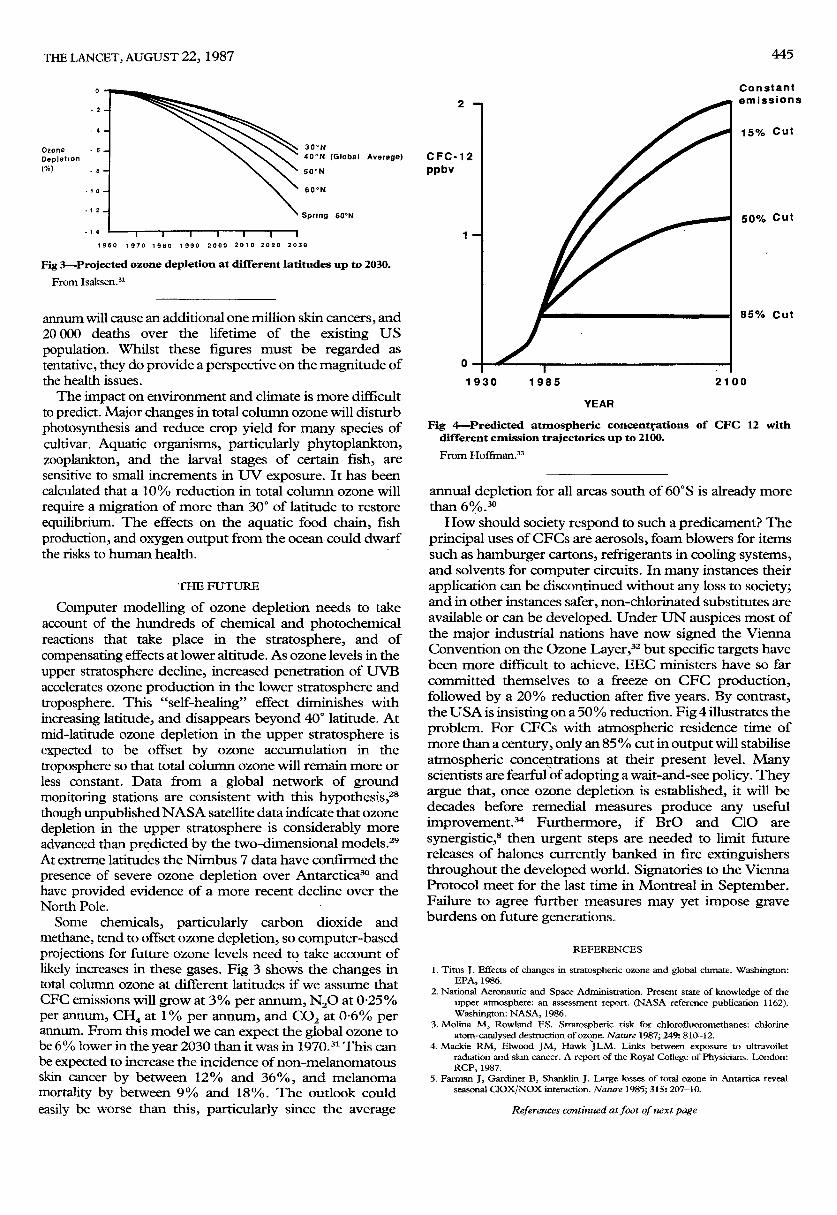
methane, tend to offset ozone depletion, so computer-basedprojections for future ozone levels need to take account oflikely increases in these gases. Fig 3 shows the changes intotal column ozone at different latitudes if we assume thatCFC emissions will grow at 3% per annum, N20 at 0-25%per annum, CH4 at 1% per annum, and CO2 at 0-6% perannum. From this model we can expect the global ozone tobe 6% lower in the year 2030 than it was in 1970.31 This canbe expected to increase the incidence of non-melanomatousskin cancer by between 12% and 36%, and melanomamortality by between 9% and 18%. The outlook couldeasily be worse than this, particularly since the average
Fig 4-Predicted atmospheric concentrations of CFC 12 withdifferent emission trajectories up to 2100.
From Hoffman.33
annual depletion for all areas south of60°S is already morethan 6%.How should society respond to such a predicament? The
principal uses of CFCs are aerosols, foam blowers for itemssuch as hamburger cartons, refrigerants in cooling systems,and solvents for computer circuits. In many instances their
application can be discontinued without any loss to society;and in other instances safer, non-chlorinated substitutes areavailable or can be developed. Under UN auspices most ofthe major industrial nations have now signed the ViennaConvention on the Ozone Layer,32 but specific targets havebeen more difficult to achieve. EEC ministers have so farcommitted themselves to a freeze on CFC production,followed by a 20% reduction after five years. By contrast,the USA is insisting on a 50 % reduction. Fig 4 illustrates theproblem. For CFCs with atmospheric residence time ofmore than a century, only an 85 % cut in output will stabiliseatmospheric concentrations at their present level. Manyscientists are fearful of adopting a wait-and-see policy. Theyargue that, once ozone depletion is established, it will bedecades before remedial measures produce any usefulimprovement.3’ Furthermore, if BrO and C10 are
synergistic,8 then urgent steps are needed to limit futurereleases of halones currently banked in fire extinguishersthroughout the developed world. Signatories to the ViennaProtocol meet for the last time in Montreal in September.Failure to agree further measures may yet impose graveburdens on future generations.
REFERENCES
1. Titus J. Effects of changes in stratospheric ozone and global climate. Washington:EPA, 1986.
2. National Aeronautic and Space Administration. Present state of knowledge of theupper atmosphere: an assessment report. (NASA reference publication 1162).Washington: NASA, 1986.
3. Molina M, Rowland FS. Stratospheric risk for chlorofluoromethanes: chlorineatom-catalysed destruction of ozone. Nature 1987; 249: 810-12.
4. Mackie RM, Elwood JM, Hawk JLM. Links between exposure to ultravoiletradiation and skin cancer. A report of the Royal College of Physicians. London:RCP, 1987.
5. Farman J, Gardiner B, Shanklin J. Large losses of total ozone in Antartica revealseasonal ClOX/NOX interaction. Nature 1985; 315: 207-10.

446
6. Cutchis P. Stratospheric ozone depletion and solar ultraviolet radiation on earth.Science 1974; 184: 13-19.
7. Cicerone R. Changes in stratospheric ozone Science 1987; 237: 35-42.8. Hills A, Cicerone R, Calved J, Birks J Kinetics of BrO and ClO reaction and
implications for stratospheric ozone. Nature 1987; 328: 405-08.9. Zafra R, Jaramillo M, Parrish A, Solomon P, Connor B, Barrett J. High concentrations
of chlorine monoxide at low altitudes in the Antarctic spring stratosphere: diurnalvariation. Nature 1987; 238: 408-11.
10. Urbach F, Epstein JH, Forbes PD, Ultraviolet carcinogenesis: experimental globaland genetic aspects. In: Fitzpatrick TB, et al, eds. Sunlight and man: normal andabnormal photobiological responses. Tokyo: University of Tokyo Press, 1974:259-83.
11. Robbins JH, Kraemer KH, Lutzner MA, Festoff BW, Coon HE. Xerodermapigmentosum: an inherited disease with sun sensitivity, multiple cutaneousneoplasms, and abnormal DNA repair. Ann Intern Med 1974; 80: 221-48.
12. McGovern V, Shaw H, Milton G, Farago G. Is malignant melanoma arising in aHutchinson’s melanotic freckle a separate disease entity? Histopathology 1980; 4:235-42.
13. Lancaster H. Some geographical aspects of the mortality from melanoma inEuropeans. Med J Aust 1956; i: 1092-87.
14. Elwood JM, Lee JAH, Walter SD. Relationship of melanoma and other skin cancermortality to latitude and ultraviolet radiation in the United States and Canada. Int JEpidemiol 1974; 3: 325-32.
15. Swerdlow AJ. Incidence of malignant melanoma of the skin in England and Wales andits relationship to sunshine. Br Med J 1979; ii: 1324-27.
16. Magnus K. Incidence of malignant melanoma of the skin in Norway 1955-1970:variations in time and space and solar radiation. Cancer 1973; 32: 1276-86.
17. Teppo L, Pakkanen M, Hakulinen T. Sunlight as a nsk factor of malignant melanomaof the skin. Cancer 1978; 41: 2018-27.
18. Eklund G, Malec E. Sunlight and incidence of cutaneous malignant melanoma: effectof latitude and domicile in Sweden. Scand J Plast Reconstr Surg 1978; 12: 321-41.
19. Lee J, Carter A. Secular trends in mortality from malignant melanoma J Natl CancerInst 1970; 45: 91-97
20. Elwood J, Lee J. Recent data on the epidemiology of malignant melanoma. SeminOncol 1975, 2: 149-54
21. Jensen O, Bolander A. Trends in malignant melanoma of the skin. World Health StatQ 1980; 33: 2-26.
22. Holman C, Mulroney C, Armstrong B. Epidemiology of preinvasive and invasivemalignant melanoma in Western Australia. Int J Cancer 1980, 25: 317-23.
23 Lee J, Strickland D. Malignant melanoma: social status and outdoor work. Br J Cancer1980; 41: 757-63.
24 Cooke K, Skegg D, Fraser J. Socioeconomic status, indoor and outdoor work. Int JCancer 1984; 34: 57-62.
25. Elwood J, Gallagher R, Davison J, Hill G. Sunburn, suntan and the nsk of cutaneousmalignant melanoma. The Western Canada Melanoma Study. Br J Cancer 1985;53: 543-49
26. Houghton A, Munster E, Viola M. Increased incidence of malignant melanoma afterpeaks of sunspot activity. Lancet 1978; i: 759-60.
27. Freeman R. Action spectrum for ultraviolet carcinogenesis Natl Cancer Inst Monogr1978; 50: 27-29.
28. US Environmental Protection Agency. An assessment of the risks of stratosphericmodification: submission to the Science Advisory Board by the Office of Air andRadiation, revised draft, January, 1987.
29. Watson R. NASA testimony to the Senate Subcommittee on Environmental
Pollution, June 10, 1986.30. Stolarski R, Krueger A, Schoeberl M, McPeters R, Newman P, Alpert J. Nimbus 7
satellite measurements of the springtime Antarctic ozone depletion. Nature 1986,322: 808-11
31. Isaksen I. Ozone perturbations studies in a 2-dimensional model with temperaturefeedback on the stratosphere included UNEP workshop, 1986.
32. United Nations Environment Programme. Vienna convention for the protection of theozone layer Nairobi: UNEP, 1985.
33. Hoffman J. The importance of knowing sooner. In- Titus J, ed. Effects of changes inthe stratosphere ozone and global change. Washington: EPA, 1986.
34. Miller A, Mintzer I. The sky is the limit: strategies for protecting the ozone layerResearch report 3, World Resources Institute, November, 1986.
In England Now
IT had been a long day. Giles had been called as dawn broke andafter a difficult journey over icy roads, he, his registrar, and thenursing team fought the age-old battle with, at least, temporarysuccess. Routine ward work followed and, after a hurried snack, hestarted his outpatient clinic. It was busier than usual and what withtrips to radiology and other departments, he was fast becoming lessthan bright-eyed and bushy-tailed. Eventually he finished, took offhis white coat, turned out the lights, and made to go home. At thatpoint he was summoned urgently to casualty. Another crisis had tobe overcome. At long last it was over. Giles sat down on one of themany comfortable wheelchairs to write his notes. Alas, thecombination of rest, warmth, and the familiar noise of the
department proved too much for him. He fell asleep.He awakened suddenly to a stentorian voice shouting in his ear.
"Arise, ye sinner! Repent your wicked ways. Give up the demondrink and you will walk again!" Startled, Giles looked up to see atall, gaunt, bearded man in uniform standing above him. He wassurrounded by a clutch of bonneted females in grey cloaks. Withoutmore ado, Giles leaped to his feet and dashed out of the front door.As he looked back he saw them all on their knees crying "Hallelujah!Another sinner saved!"
* * *
THERE was a period in my young life-I was 10 or 11 at the time,not yet in long trousers-when I was irresistibly attractive to dogs,and it lasted several months. Any stray dog on the streets, catchingsight of me in the distance, would scamper to my side and follow mehome. There, assuming that I did not let him pass through the frontgarden gate, he would hang about on the pavement awaiting mynext appearance. To pass the time he might have a fight or two withhis rivals. This was tiresome enough, but much worse was when heleapt up, embraced my leg between his own front legs, like a pair ofchopsticks, and humped his back to and fro rhythmically. I, ofcourse, did not know what it was all about-possibly took it as acompliment-and a well-directed kick from some nearby adultwould dislodge the animal before he had time to squirt his semen onto my socks. It was even more embarrassing when I was visitingfriends and their pet greeted me with the same salutation. I had noreason to think I smelled any differently from my siblings. I washed
with the same soap and had my bath every evening. Yet they wereimmune from such attentions. Today, slightly more knowledge-able, I must conclude that during my prepubescence I was
emitting a pheromone, similar or even identical to that of a bitch onheat and guaranteed to inflame any male dog within a mile.The phase ended and was forgotten until I was 19 or so when
unwittingly I incurred the enmity of swans. Not just one particularswan, but swans in general, whether at Highgate Ponds or on theNorfolk Broads. An apparently pacific swan, doing the beautifulthings that swans are so good at, on catching sight of me in the fardistance, would instantly be transformed into a FruminousBandersnatch. Arising to its full height, with wings outstretchedand neck thrust forward, it would rush across the water hissing like apressure-cooker. I never stood my ground. A blow from a swan’swing, I had been told, could break a chap’s arm. So I fled. Once onBarton Broad I had to cower out of sight in the sternsheets of asailing dinghy. The frustrated brute vented its anger by pecking atthe boat’s hull before sailing beautifully away.
I do not know whether I have lost this strange magnetism forswans ... I have never put it to the test. The next village, throughwhich I sometimes drive, has a mill-pond with a couple of idleswans messing about on it. I often say that one day I shall stop andget out and make faces at them-leaving the car door open, just incase. But I know I never shall.
* * *
MEDICAL literature is written in an objective mode. All personalqualities are suppressed and the subjective expression is frownedupon. I remember a senior colleague stating "Take out those ’1’s!"as he reviewed an early paper of mine: " ’1’ detracts from the
message and focuses attention on the author in place of the story".Consequently, for years I have written in the third person or even inpassive construction to avoid the dreaded "I".
This was recalled as I recognised why I enjoy In England Now. Itis a series of observations usually couched in the first person. "I"after "I" tramps across the paragraphs telling us what happened. Itmay be associated with the rarest of medical words: "me" or"mine". This section of The Lancet is a charming personal oasis in adrab third-person desert. I feel for the author of those vignettesabout Giles, the all-purpose medical man, since the author chose towrite through Giles, missing the direct possession of his creation.However, now and again irrepressible Giles breaks forth with an"I" and then I know everyone feels better: even an "I" can be
enjoyed secondhand.