Embed Size (px)
Citation preview

A
a
Pfa(
aP5(
r©
K
R
a
icsrG
0d
Annales de Cardiologie et d’Angéiologie 61 (2012) 20–26
Original article
Plaque rupture and morphological characteristics of the culprit lesion inacute coronary syndromes without significant angiographic lesion:
Analysis by intravascular ultrasound
Rupture de plaque et caractéristiques morphologiques de la lésion coupable au décours dessyndromes coronariens aigus sans lésion angiographiquement significative:
étude par échographie endocoronaire
H. Ouldzein ∗, M. Elbaz , J. Roncalli , R. Cagnac , D. Carrié , J. Puel †, M.-J. Alibelli-Chemarin †Fédération de cardiologie, service de cardiologie B, pôle cardiovasculaire et métabolique, hôpital de Rangueil, 31059 Toulouse cedex 9, France
Received 13 July 2011; accepted 24 July 2011Available online 22 August 2011
bstract
Purpose. – To evaluate by intravascular ultrasound (IVUS) the characteristics of the culprit lesion with plaque rupture without significantngiographic stenosis after acute coronary syndromes (ACS).
Patients and methods. – After ACS, IVUS was performed in 68 patients (46.8 years ± 11.9) without significant angiographic stenosis (31 ± 15%).laque rupture was defined as a cavity within the plaque, communicating with the arterial lumen and having an overlying residual fibrous capragment. Qualitative analysis defined the type of plaque, and quantitative analysis evaluated plaque plus media area, plaque volume, plaque burden,nd arterial remodeling index. Patients were divided into two groups: Group I with plaque rupture (25 patients) and Group II without plaque rupture43 patients).
Results. – All patients with rupture showed soft or mixed plaque but no calcified plaque. In Group I, plaque rupture was associated with larger plaque burden (49.8 ± 12.3% vs. 39.8 ± 12.1%, P < .0005), a more significant plaque plus media area (7.44 ± 2.9 vs. 5.24 ± 2.4 mm2,
< .001), a greater plaque volume (151.9 ± 103.4 vs. 99.2 ± 81.6 mm3, P < .007), and a higher ratio of plaque volume over length (8.0 ± 3.8 vs..6 ± 3.7 mm3/mm, P < .003). In Group I, positive remodeling was more frequent than intermediate remodeling (P < .03) or negative remodelingP < .005). In Group II, there was no significant difference between the three types of remodeling.
Conclusion. – The plaque ruptures responsible for ACS frequently appear on voluminous plaques with a large plaque burden and positive arterialemodeling.
2011 Elsevier Masson SAS. All rights reserved.
eywords: Intravascular ultrasound; Arterial remodeling; Plaque rupture; Acute coronary syndrome
ésumé
Objectif. – Étudier par l’échographie endocoronaire les caractéristiques morphologiques de la lésion rompue au décours d’un syndrome coronarienigu sans lésion angiographique significative.
Patients et méthodes. – Une échographie endocoronaire a été réalisée chez 68 patients (46.8 ± 11,9 ans) après un SCA (21 IDM et 47 angornstable) sans sténose angiographique significative (31% ± 15). La rupture était authentifiée par la présence d’une cavité au sein de la plaque,
ommuniquant avec la lumière artérielle et recouverte d’un fragment de chape fibreuse. L’analyse qualitative de la plaque a permis de préciseron type échographique, l’analyse quantitative a évalué la surface plaque + média, le volume de plaque, le comblement athéromateux et l’index deemodelage artériel au niveau de la lésion responsable du SCA. Les patients ont été divisés en deux groupes : Groupe I avec rupture (25 patients),roupe II sans rupture (43 patients).∗ Corresponding author.E-mail address: [email protected] (H. Ouldzein).
† Deceased authors.
003-3928/$ – see front matter © 2011 Elsevier Masson SAS. All rights reserved.oi:10.1016/j.ancard.2011.07.011
cplép
a©
M
1
aliuoiNootTlwa
2
2
ttaCns
Fs
H. Ouldzein et al. / Annales de Cardiologie et d’Angéiologie 61 (2012) 20–26 21
Résultats. – Les patients avec rupture présentaient tous une plaque molle ou mixte, non calcifiée. La rupture de plaque était associée à unomblement athéromateux plus important dans le groupe I (49,8 ± 12,3% vs 39,8 ± 12,1%, p < 0,0005). Il en était de même pour la surfacelaque + media (7,4 ± 2,9 mm2 vs 5,2 ± 2,4 mm2, p < 0,001), pour le volume de plaque (151,9 ± 103,4 mm3 vs 99,2 ± 81,6 mm3, p < 0,007) et poure rapport volume de plaque sur longueur plus élevé (8,0 ± 4,1 mm3/mm vs 5,9 ± 3,7 mm3/mm, p < 0,003). Dans le groupe I, le remodelage positiftait plus fréquemment retrouvé que le remodelage intermédiaire (p < 0,03) ou que le remodelage négatif (p < 0,005). Dans le groupe II, il n’existaitas de différence significative entre les trois types de remodelage.
Conclusion. – Les ruptures, responsables d’un SCA, surviennent essentiellement sur des plaques volumineuses, avec important comblementthéromateux et remodelage artériel positif.
2011 Elsevier Masson SAS. Tous droits réservés.
thie
2
boUmrlorppaqi
2
rpcnsc
ots clés : Ultrasons ; Angiographie ; Imagerie ; Athérosclérose ; Coronaropa
. Introduction
Previous studies have shown strong correlations betweentheromatous plaque rupture and angiographically complexesions [1], and plaque rupture is a factor for poor prognosisn acute coronary syndromes (ACS) [2]. Recent intravascularltrasound (IVUS) studies [3–6] have described the frequencyf plaque rupture in ACS (20–40%) [3–8] and the possibil-ty of multiple ruptured coronary other than the culprit lesion.evertheless, plaque ruptures were rarely observed by IVUSn coronary arteries without significant stenosis (percentagef stenosis ≤ 50%) [9–12] and the morphological characteris-ics of the ruptured plaque have not yet been fully described.he aim of this study was to evaluate by IVUS the morpho-
ogical and quantitative characteristics of the culprit lesionith plaque rupture without significant angiographic stenosis
fter ACS.
. Patients and methods
.1. Patient population
Sixty-eight ACS patients (45 male and 23 female) with lesshan 50% stenosis were included: 21 acute myocardial infarc-ion (MI) and 47 unstable angina (UA). All were treated withspirin and clopidogrel prior to the time of the IVUS procedure.
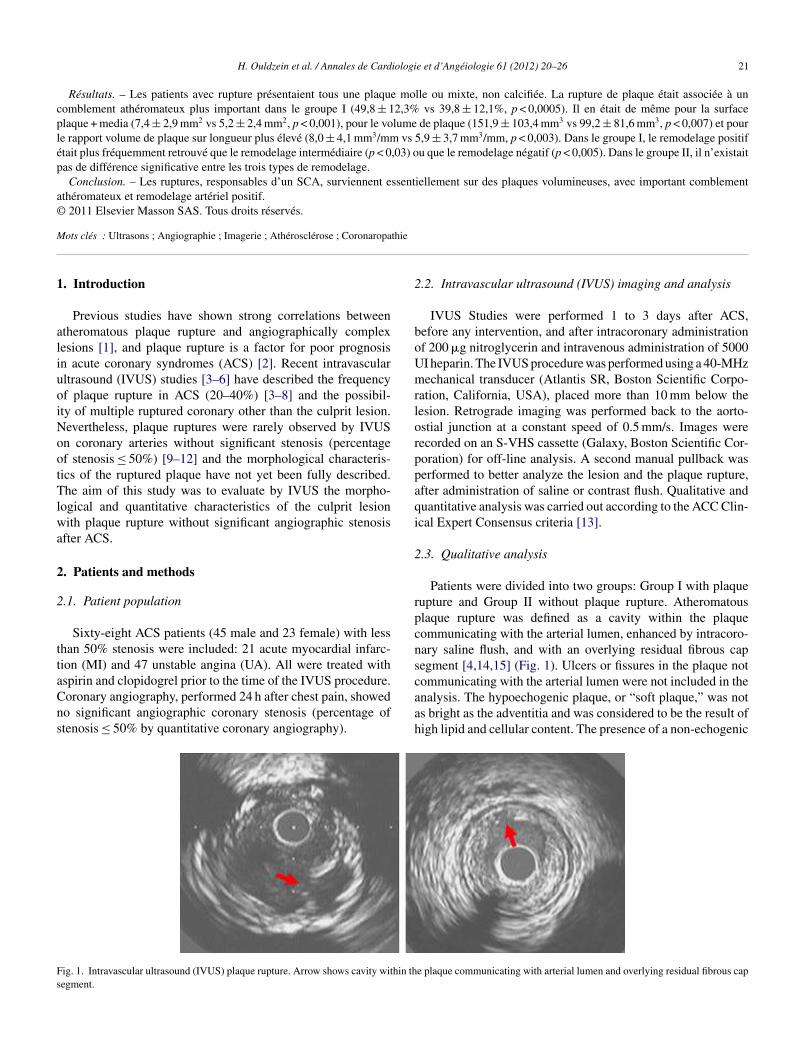
oronary angiography, performed 24 h after chest pain, showedo significant angiographic coronary stenosis (percentage oftenosis ≤ 50% by quantitative coronary angiography).ig. 1. Intravascular ultrasound (IVUS) plaque rupture. Arrow shows cavity within thegment.
aah
.2. Intravascular ultrasound (IVUS) imaging and analysis
IVUS Studies were performed 1 to 3 days after ACS,efore any intervention, and after intracoronary administrationf 200 �g nitroglycerin and intravenous administration of 5000I heparin. The IVUS procedure was performed using a 40-MHzechanical transducer (Atlantis SR, Boston Scientific Corpo-
ation, California, USA), placed more than 10 mm below theesion. Retrograde imaging was performed back to the aorto-stial junction at a constant speed of 0.5 mm/s. Images wereecorded on an S-VHS cassette (Galaxy, Boston Scientific Cor-oration) for off-line analysis. A second manual pullback waserformed to better analyze the lesion and the plaque rupture,fter administration of saline or contrast flush. Qualitative anduantitative analysis was carried out according to the ACC Clin-cal Expert Consensus criteria [13].
.3. Qualitative analysis
Patients were divided into two groups: Group I with plaqueupture and Group II without plaque rupture. Atheromatouslaque rupture was defined as a cavity within the plaqueommunicating with the arterial lumen, enhanced by intracoro-ary saline flush, and with an overlying residual fibrous capegment [4,14,15] (Fig. 1). Ulcers or fissures in the plaque notommunicating with the arterial lumen were not included in the
e plaque communicating with arterial lumen and overlying residual fibrous cap
nalysis. The hypoechogenic plaque, or “soft plaque,” was nots bright as the adventitia and was considered to be the result ofigh lipid and cellular content. The presence of a non-echogenic
22 H. Ouldzein et al. / Annales de Cardiologie et d’Angéiologie 61 (2012) 20–26
F l the cd al anp
zi“wadctms
2
qScr
aasdslas
mmt
epmd(noLL
Eplaroewapsiweo
2
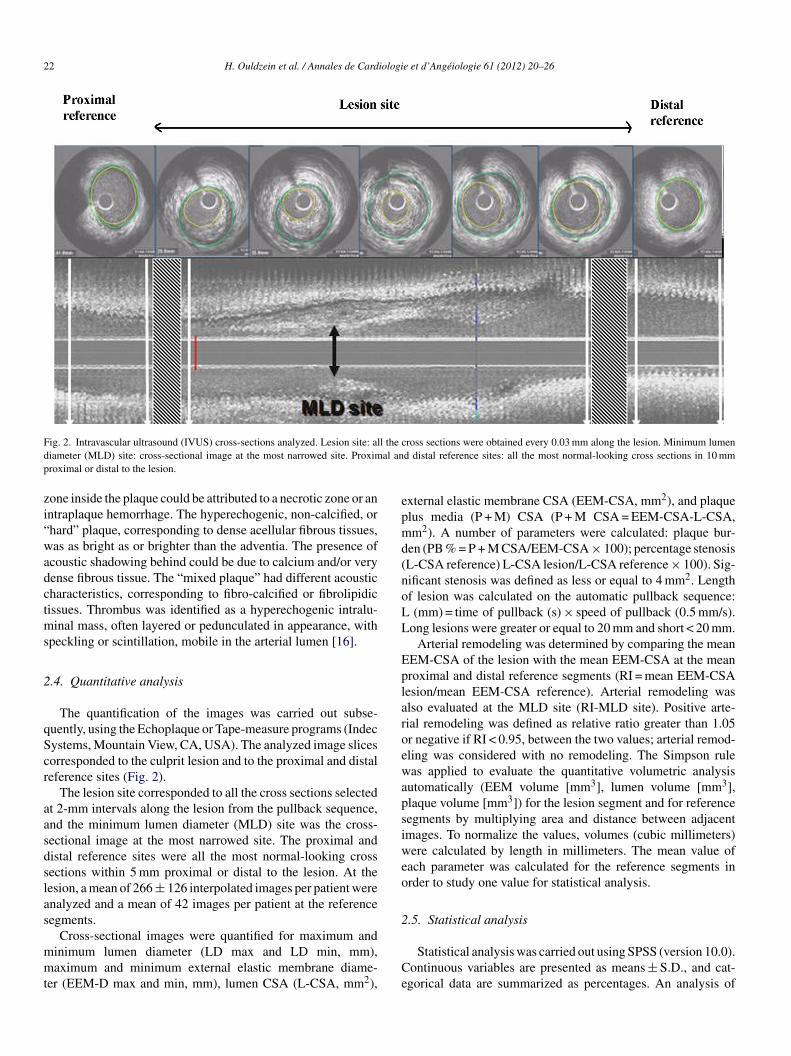
ig. 2. Intravascular ultrasound (IVUS) cross-sections analyzed. Lesion site: aliameter (MLD) site: cross-sectional image at the most narrowed site. Proximroximal or distal to the lesion.
one inside the plaque could be attributed to a necrotic zone or anntraplaque hemorrhage. The hyperechogenic, non-calcified, orhard” plaque, corresponding to dense acellular fibrous tissues,as as bright as or brighter than the adventia. The presence of
coustic shadowing behind could be due to calcium and/or veryense fibrous tissue. The “mixed plaque” had different acousticharacteristics, corresponding to fibro-calcified or fibrolipidicissues. Thrombus was identified as a hyperechogenic intralu-inal mass, often layered or pedunculated in appearance, with
peckling or scintillation, mobile in the arterial lumen [16].
.4. Quantitative analysis
The quantification of the images was carried out subse-uently, using the Echoplaque or Tape-measure programs (Indecystems, Mountain View, CA, USA). The analyzed image slicesorresponded to the culprit lesion and to the proximal and distaleference sites (Fig. 2).
The lesion site corresponded to all the cross sections selectedt 2-mm intervals along the lesion from the pullback sequence,nd the minimum lumen diameter (MLD) site was the cross-ectional image at the most narrowed site. The proximal andistal reference sites were all the most normal-looking crossections within 5 mm proximal or distal to the lesion. At theesion, a mean of 266 ± 126 interpolated images per patient werenalyzed and a mean of 42 images per patient at the referenceegments.
Cross-sectional images were quantified for maximum andinimum lumen diameter (LD max and LD min, mm),aximum and minimum external elastic membrane diame-
er (EEM-D max and min, mm), lumen CSA (L-CSA, mm2),Ce
ross sections were obtained every 0.03 mm along the lesion. Minimum lumend distal reference sites: all the most normal-looking cross sections in 10 mm
xternal elastic membrane CSA (EEM-CSA, mm2), and plaquelus media (P + M) CSA (P + M CSA = EEM-CSA-L-CSA,m2). A number of parameters were calculated: plaque bur-
en (PB % = P + M CSA/EEM-CSA × 100); percentage stenosisL-CSA reference) L-CSA lesion/L-CSA reference × 100). Sig-ificant stenosis was defined as less or equal to 4 mm2. Lengthf lesion was calculated on the automatic pullback sequence:
(mm) = time of pullback (s) × speed of pullback (0.5 mm/s).ong lesions were greater or equal to 20 mm and short < 20 mm.
Arterial remodeling was determined by comparing the meanEM-CSA of the lesion with the mean EEM-CSA at the meanroximal and distal reference segments (RI = mean EEM-CSAesion/mean EEM-CSA reference). Arterial remodeling waslso evaluated at the MLD site (RI-MLD site). Positive arte-ial remodeling was defined as relative ratio greater than 1.05r negative if RI < 0.95, between the two values; arterial remod-ling was considered with no remodeling. The Simpson ruleas applied to evaluate the quantitative volumetric analysis
utomatically (EEM volume [mm3], lumen volume [mm3],laque volume [mm3]) for the lesion segment and for referenceegments by multiplying area and distance between adjacentmages. To normalize the values, volumes (cubic millimeters)ere calculated by length in millimeters. The mean value of
ach parameter was calculated for the reference segments inrder to study one value for statistical analysis.
.5. Statistical analysis
Statistical analysis was carried out using SPSS (version 10.0).ontinuous variables are presented as means ± S.D., and cat-gorical data are summarized as percentages. An analysis of
H. Ouldzein et al. / Annales de Cardiologie et d’Angéiologie 61 (2012) 20–26 23
Table 1Demographic characteristics.
All patients (n = 68) Group I (n = 25) Group II (n = 43) P value
Mean age (years) 46.8 ± 11.9 45.3 ± 12.1 47.6 ± 11.9 nsGender, n (%) ns
Male 45 (66.2) 19 (76.0) 26 (60.5)Female 23 (33.8) 6 (24.0) 17 (39.5)
Risk factors, n (%)Current smocking 47 (69.1) 16 (64.0) 31 (72.1) nsDiabetes mellitus 3 (4.4) 0 3 (7.0) nsHypercholesteroemia 18 (26.5) 5 (20.0) 13 (30.2) nsHypertension 14 (20.6) 4 (16.0) 10 (23.3) ns
Symptoms, n (%) nsMI 31 (45.6) 14 (56.0) 17 (39.5)UA 37 (54.4) 11 (44.0) 26 (60.5)
Coronary angiography nsLeft anterior descending, n (%) 42 (61.8) 14 (56.0) 28 (65.1)Right coronary, n (%) 20 (29.4) 10 (40.0) 10 (23.3)Circumflex, n (%) 6 (8.8) 1 (4.0) 5 (11.6)
P
M
vtMabBP
3
a
3
yj
aCT2
3
bewPfw
TI
T
ICTT
N
V
ercentage stenosis (%) 31 ± 15
I: acute myocardial infarction; UA: unstable angina
ariance (ANOVA) was computed to compare the means of con-inuous variables, and a nonparametric test (Kruskal–Wallis or
ann–Whitney test) was used when the distribution of the vari-ble was not normal or when variances differed significantlyetween groups (variance homogeneity was tested using theartlett �2 test). Percentages were compared with the �2 test. A-value below 0.05 was considered as significant.
. Results
The results are shown for all patients: Group I with rupturend Group II without rupture.
.1. Clinical results
The mean age of the studied population was 46.8 ± 11.9ears (range, 22–79 years) with more male than female sub-ects (Table 1). Plaque ruptures were found more frequently after
tgt1
able 2ntravascular ultrasound (IVUS): qualitative data.
All patients (n = 68) G
ype of plaque
Normal 3 (4.4)
Nonechogenic (soft) 32 (47.1)
Hyperechogenic (hard) 5 (7.4)
Mixed 28 (41.2)
ntimal thickening 17 (25.0)
alcification 6 (8.8)
hrombus 26 (38.2)
ype of atheromaFocal disease 35 (51.5)
Diffuse disease 30 (44.1)
o. of lesions
1 61 (89.7)
2 4 (5.9)
alues are shown as n (%).a Test of Mann–Whitney.
36 ± 13 28 ± 15 < .042
cute myocardial infarction (56%), but not significantly more.oronary artery lesions were distributed equally in three groups.he percentage of stenosis was greater in Group I (36 ± 13% vs.8 ± 15%, P < .04).
.2. Intravascular ultrasound (IVUS) results
Qualitatively (Table 2), no significant difference was foundetween the two groups in the type of plaque, which wasssentially hypo-echogenic or soft and mixed. Diffuse atheromaas statistically more frequent in Group I (64.0% vs. 32.6%,
< .008). For both types of SCA (MI or UA), plaque rupture wasound in 25 patients (36.8%), which was significantly associatedith thrombus in Group I (68% vs. 21%, P < .0005). Quantita-
ively (Table 3), the length of the lesion was the same in bothroups (19.3 ± 9.0 vs. 17.6 ± 8.9 mm, ns). (P + M) CSA at thearget lesion was greater in Group I (7.4 ± 2.9 vs. 5.2 ± 2.4 mm83 2, P < .001) with plaque burden significantly greater
roup I (n = 25) Group II (n = 43) P value
ns0 (0.0) 3 (7.0)
13 (52.0) 19 (44.2)0 (0.0) 5 (11.6)
12 (48.0) 16 (37.2)6 (24.0) 11 (25.6) ns3 (12.0) 3 (7.0) ns
17 (68.0) 9 (20.9) < .0005< .008a
9 (36.0) 26 (60.5)16 (64.0) 14 (32.6)
nsa
23 (92.0) 38 (88.4)2 (8.0) 2 (4.7)
24 H. Ouldzein et al. / Annales de Cardiologie et d’Angéiologie 61 (2012) 20–26
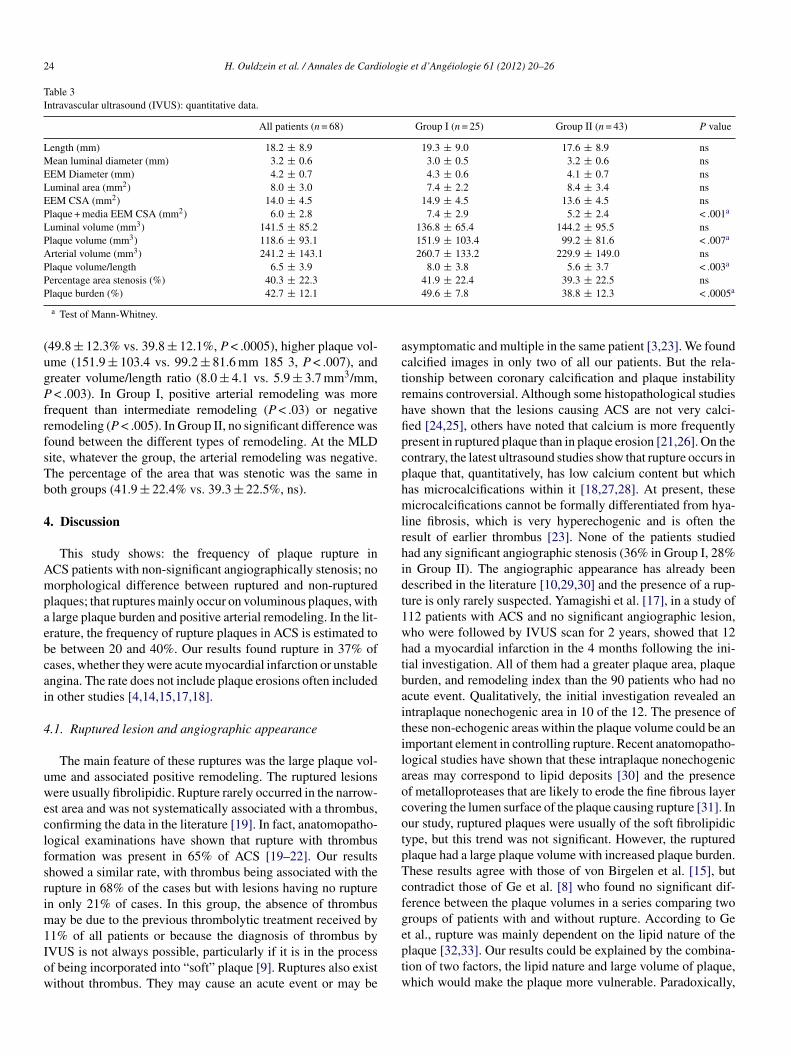
Table 3Intravascular ultrasound (IVUS): quantitative data.
All patients (n = 68) Group I (n = 25) Group II (n = 43) P value
Length (mm) 18.2 ± 8.9 19.3 ± 9.0 17.6 ± 8.9 nsMean luminal diameter (mm) 3.2 ± 0.6 3.0 ± 0.5 3.2 ± 0.6 nsEEM Diameter (mm) 4.2 ± 0.7 4.3 ± 0.6 4.1 ± 0.7 nsLuminal area (mm2) 8.0 ± 3.0 7.4 ± 2.2 8.4 ± 3.4 nsEEM CSA (mm2) 14.0 ± 4.5 14.9 ± 4.5 13.6 ± 4.5 nsPlaque + media EEM CSA (mm2) 6.0 ± 2.8 7.4 ± 2.9 5.2 ± 2.4 < .001a
Luminal volume (mm3) 141.5 ± 85.2 136.8 ± 65.4 144.2 ± 95.5 nsPlaque volume (mm3) 118.6 ± 93.1 151.9 ± 103.4 99.2 ± 81.6 < .007a
Arterial volume (mm3) 241.2 ± 143.1 260.7 ± 133.2 229.9 ± 149.0 nsPlaque volume/length 6.5 ± 3.9 8.0 ± 3.8 5.6 ± 3.7 < .003a
Percentage area stenosis (%) 40.3 ± 22.3 41.9 ± 22.4 39.3 ± 22.5 nsP a
(ugPfrfsTb
4
Ampaebcai
4
uweclfsrim1Iow
actrhfipcphmlrhidt1whtbaitilaocotpTcfge
laque burden (%) 42.7 ± 12.1
a Test of Mann-Whitney.
49.8 ± 12.3% vs. 39.8 ± 12.1%, P < .0005), higher plaque vol-me (151.9 ± 103.4 vs. 99.2 ± 81.6 mm 185 3, P < .007), andreater volume/length ratio (8.0 ± 4.1 vs. 5.9 ± 3.7 mm3/mm,
< .003). In Group I, positive arterial remodeling was morerequent than intermediate remodeling (P < .03) or negativeemodeling (P < .005). In Group II, no significant difference wasound between the different types of remodeling. At the MLDite, whatever the group, the arterial remodeling was negative.he percentage of the area that was stenotic was the same inoth groups (41.9 ± 22.4% vs. 39.3 ± 22.5%, ns).
. Discussion
This study shows: the frequency of plaque rupture inCS patients with non-significant angiographically stenosis; noorphological difference between ruptured and non-ruptured
laques; that ruptures mainly occur on voluminous plaques, with large plaque burden and positive arterial remodeling. In the lit-rature, the frequency of rupture plaques in ACS is estimated toe between 20 and 40%. Our results found rupture in 37% ofases, whether they were acute myocardial infarction or unstablengina. The rate does not include plaque erosions often includedn other studies [4,14,15,17,18].
.1. Ruptured lesion and angiographic appearance
The main feature of these ruptures was the large plaque vol-me and associated positive remodeling. The ruptured lesionsere usually fibrolipidic. Rupture rarely occurred in the narrow-
st area and was not systematically associated with a thrombus,onfirming the data in the literature [19]. In fact, anatomopatho-ogical examinations have shown that rupture with thrombusormation was present in 65% of ACS [19–22]. Our resultshowed a similar rate, with thrombus being associated with theupture in 68% of the cases but with lesions having no rupturen only 21% of cases. In this group, the absence of thrombus
ay be due to the previous thrombolytic treatment received by
1% of all patients or because the diagnosis of thrombus byVUS is not always possible, particularly if it is in the processf being incorporated into “soft” plaque [9]. Ruptures also existithout thrombus. They may cause an acute event or may beptw
49.6 ± 7.8 38.8 ± 12.3 < .0005
symptomatic and multiple in the same patient [3,23]. We foundalcified images in only two of all our patients. But the rela-ionship between coronary calcification and plaque instabilityemains controversial. Although some histopathological studiesave shown that the lesions causing ACS are not very calci-ed [24,25], others have noted that calcium is more frequentlyresent in ruptured plaque than in plaque erosion [21,26]. On theontrary, the latest ultrasound studies show that rupture occurs inlaque that, quantitatively, has low calcium content but whichas microcalcifications within it [18,27,28]. At present, theseicrocalcifications cannot be formally differentiated from hya-
ine fibrosis, which is very hyperechogenic and is often theesult of earlier thrombus [23]. None of the patients studiedad any significant angiographic stenosis (36% in Group I, 28%n Group II). The angiographic appearance has already beenescribed in the literature [10,29,30] and the presence of a rup-ure is only rarely suspected. Yamagishi et al. [17], in a study of12 patients with ACS and no significant angiographic lesion,ho were followed by IVUS scan for 2 years, showed that 12ad a myocardial infarction in the 4 months following the ini-ial investigation. All of them had a greater plaque area, plaqueurden, and remodeling index than the 90 patients who had nocute event. Qualitatively, the initial investigation revealed anntraplaque nonechogenic area in 10 of the 12. The presence ofhese non-echogenic areas within the plaque volume could be anmportant element in controlling rupture. Recent anatomopatho-ogical studies have shown that these intraplaque nonechogenicreas may correspond to lipid deposits [30] and the presencef metalloproteases that are likely to erode the fine fibrous layerovering the lumen surface of the plaque causing rupture [31]. Inur study, ruptured plaques were usually of the soft fibrolipidicype, but this trend was not significant. However, the rupturedlaque had a large plaque volume with increased plaque burden.hese results agree with those of von Birgelen et al. [15], butontradict those of Ge et al. [8] who found no significant dif-erence between the plaque volumes in a series comparing tworoups of patients with and without rupture. According to Get al., rupture was mainly dependent on the lipid nature of the
laque [32,33]. Our results could be explained by the combina-ion of two factors, the lipid nature and large volume of plaque,hich would make the plaque more vulnerable. Paradoxically,
iologi
tnh
4
rrttaciwndco
5
s“p
6
adfttplnb
D
c
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
H. Ouldzein et al. / Annales de Card
he ruptured plaque was not in the area of the artery with thearrowest stenosis. This phenomenon is possibly explained byigh positive arterial remodeling in the ruptured areas.
.2. Arterial remodeling
When an angiographic lesion develops, the compensationemodeling described by Glacov et al. [34] preserves the arte-ial lumen as long as the plaque surface is less than 40% ofhe arterial surface. As soon as the plaque volume increases,he compensation mechanism stops acting and the remodeledtheroma becomes more sensitive to mechanical forces, whichan cause the rupture [35,36]. So positive remodeling [35–37]s often associated with ruptured plaque [4,13,15,17,37–39],hich agrees with our findings. But remodeling is not homoge-ous all along the artery, because in the area where the lumeniameter and lumen surface are smallest, there may be arterialonstriction. In cases of ACS without plaque rupture, all typesf remodeling are seen.
. Conclusion
Plaque rupture is common after ACS in patients withoutignificant angiographic stenosis. It occurs most frequently insoft,” fibrolipidic plaque, with a large plaque volume andlaque burden.
. Limitations of the study
The main limitations of this study are its small sample sizend the absence of a control group with a stable coronary syn-rome. There may be errors in thrombus detection due to theact that some patients were treated with thrombolytics beforeheir ultrasound. Also, only large and clearly identifiable rup-ures were selected. Smaller ruptures may have gone unnoticed,articularly if they were hidden by thrombus. Lastly, as far asong lesions are concerned, when the rupture was not in thearrowest region of the stenosis, it was difficult to differentiateetween areas that do and do not cause ACS.
isclosure of interest
The authors declare that they have no conflicts of interestoncerning this article.
eferences
[1] Levin DC, Fullon JT. Significance of the angiography morphologyof localized coronary stenoses: histopathologic correlations. Circulation1982;66:316–20 [310].
[2] Lee SG, Lee CW, Hong MK, Kim JJ, Park SW, Park SJ. Change of multiplecomplex coronary plaques in patients with acute myocardial infarction: astudy with coronary angiography. Am Heart J 2004;147:281–6.
[3] Rioufol G, Finet G, Ginon I, André-Fouët X, Rossi R, Vialle E, et al.Multiple atherosclerotic plaque rupture in acute coronary syndrome: a
three-vessel intravascular ultrasound study. Circulation 2002;106:804–8.[4] Maehara A, Mintz GS, Bui AB, Walter OR, Castagna MT, Canos D, et al.Morphologic and angiographic features of coronary plaque rupture detectedby intravascular ultrasound. J Am Coll Cardiol 2002;40:904–10.
[
e et d’Angéiologie 61 (2012) 20–26 25
[5] Mintz GS, Maehara A, Bui AB, Weissman NJ. Multiple versus single coro-nary plaques ruptures detected by intravascular ultrasound in stable anunstable angina pectoris and in acute myocardial infarction. Am J Cardiol2003;91:1333–5.
[6] Fujii K, Kobayashi Y, Mintz GS, Takebayashi H, Dangas G, Moussa I,et al. Intravascular ultrasound assessment of ulcerated ruptured plaques: acomparison of culprit and nonculprit lesions of patients with acute coronarysyndromes and in patients without acute coronary syndromes. Circulation2003;108:2473–8.
[7] Fukuda D, Kawarabayashi T, Tanaka A, Nishibori Y, Taguchi H, Nishida Y,et al. Lesion characteristics of acute myocardial infarction: an investigationwith intravascular ultrasound. Heart 2001;85:402–6.
[8] Ge J, Chirillo F, Schwedtmann J, Görge G, Haude M, Baumgart D, et al.Screening of ruptured plaques in patients with coronary artery disease byintravascular ultrasound. Heart 1999;81:621–7.
[9] Fishbein MC, Siegel RJ. How big are coronary atherosclerotic plaque thatrupture? Circulation 1996;94:2662–6.
10] Ambrose JA, Tanneebaum MA, Alexopoulos D. Angiographic progressionof coronary artery disease and the development of myocardial infarction. JAm Coll Cardiol 1988;12:56–62.
11] Giroud D, Li JM, Urban P, Meier B, Rutishauser W. Relation of the site ofacute myocardial infarction to the most severe coronary arterial stenosis atprior angiography. Am J Cardiol 1992;69:729–32.
12] Nissen SE, Yock P. Intravascular ultrasound: novel pathophysiologicalinsights and current clinical applications. Circulation 2001;103:604–16.
13] Mintz GS, Nissen SE, Anderson WD, Bailey SR, Erbel R, Fitzgerald PJ,et al. ACC Clinical Expert Consensus Document on standards for the acqui-sition, measurement and reporting of intravascular ultrasound studies: areport of the American College of Cardiology Task Force on ClinicalExpert Consensus Documents (Committee to Develop a Clinical ExpertConsensus Document on Standards for Acquisition, Measurement andReporting of Intravascular Ultrasound Studies [IVUS]). J Am Coll Cardiol2001;37:1478–92.
14] Nagai T, Luo H, Atar S, Lepor NE, Fishbein MC, Siegel RJ. Intravascularultrasound imaging of ruptured atherosclerotic plaques in coronary arteries.Am J Cardiol 1999;83:135–7.
15] von Birgelen C, Klinkhart W, Mintz GS, Papatheodorou A, Herrmann J,Baumgart D, et al. Plaque distribution and vascular remodeling of rup-tured and nonruptured coronary plaques in the same vessel: an intravascularultrasound study in vivo. J Am Coll Cardiol 2001;37:1864–70.
16] Chemarin-Alibelli MJ, Pieraggi MT, Elbaz M, Carrie D, Fourcade J, PuelJ, et al. Identification of coronary thrombus after myocardial infarction byintracoronary ultrasound compared with histology of tissues sampled byatherectomy. Am J Cardiol 1996;77:344–9.
17] Yamagishi M, Terashima M, Awano K, Kijima M, Nakatani S, Daikoku S,et al. Morphology of vulnerable coronary plaque: insights from follow-upof patients examined byintravascular ultrasound before an acute coronarysyndrome. J Am Coll Cardiol 2000;35:106–11.
18] Rasheed Q, Nair R, Hodgson JM. Correlation of intracoronary ultrasoundplaque characteristics in atherosclerotic coronary artery disease patientswith clinical variables. Am J Cardiol 1994;73:753–8.
19] Davies MJ, Thomas AC. Plaque fissuring–the cause of acute myocar-dial infarction, sudden ischaemic death, and crescendo angina. Br HeartJ 1985;53:363–73.
20] Falk E. Morphologic features of unstable atherothrombotic plaques under-lying acute coronary syndromes. Am J Cardiol 1989;63:114E–20E.
21] Farb A, Burke AP, Tang AL, Liang TY, Mannan P, Smialek J, et al. Coronaryplaque erosion without rupture into a lipid core. A frequent cause of coro-nary thrombosis in sudden coronary death. Circulation 1996;93:1354–63.
22] Virnani E, Kolodgie FD, Burke AP, Schwartz SM. Lessons from suddencoronary death. A comprehensive morphological classification scheme foratherosclerotic lesions. Arterioscler Thromb Vasc Biol 2000;20:1262–75.
23] Rioufol G, Gilard M, Finet G, Ginon I, Boschat J, Andre-Fouêt X.Evolution of spontaneous atherosclerotic plaque rupture with medical
treatment. Long-term follow-up with intravascular ultrasound. Circulation2004;110:2875–80.24] Gertz G, Roberts WC. Hemodynamic shear force in rupture of coronaryarterial atherosclerotic plaques. Am J Cardiol 1990;66:1368–72.

2 iologi
[
[
[
[
[
[
[
[
[[
[
[
[
[
6 H. Ouldzein et al. / Annales de Card
25] Cheng GC, Loree HM, Kamm RD, FishbeinMC, Lee RT. Distribu-tion of circumferential stress in ruptured and stable atheroscleroticlesions. A structural analysis with histopathological correlation. Circulation1993;87:1179–87.
26] Burke AP, Taylor A, Farb A, Malcom GT, Virmani R. Coronary calcificationinsights from sudden coronary death victims. Z Kardiol 2000;89(Suppl.2):49–53.
27] Nakamura M, Nishikawa H, Mukai S, Setsuda M, Nakajima K, TamadaH, et al. Impact of coronary artery remodeling on clinical presentationof coronary artery disease an intravascular ultrasound study. J Am CollCardiol 2001;37:63–9.
28] Fujii K, Carlier SG, Mintz GS, Takebayashi H, Yasuda T, Costa RA, et al.Intravascular ultrasound study of patterns of calcium in ruptured coronaryplaques. Am J Cardiol 2005;96:352–7.
29] Little WC, Constantinescu M, Applegate RJ, Kutcher MA, Burrows MT,Kahl FR, et al. Can coronary angiography predict the site of a subsequentmyocardial infarction in patients with mild-to-moderate coronary arterydisease? Circulation 1988;78:1157–66.
30] Gronholdt ML, Nordestgaard BG, Wiebe BM, Wilhjelm JE, Sillesen H.Echo-lucency of computerized ultrasound images of carotid atheroscleroticplaques are associated with increased levels of triglyceride-rich lipoproteinsas well as increased plaque lipid content. Circulation 1998;97:34–40.
31] Shah PK, Falk E, Badimon JJ, Fernandez-Ortiz A, MailhacA, Villareal-
levy G, et al. Human monocyte-derived macrophages induce collagenbreakdown in fibrous caps of atherosclerotic plaques. Potential role ofmatrix-degrading metalloproteinases and implications for plaque rupture.Circulation 1995;92:1565–9.[
e et d’Angéiologie 61 (2012) 20–26
32] Davies MJ, Bland MJ, Hangartner JR, Angelini A, Thomas AC. Factorsinfluencing the presence or absence of acute coronary thrombi in suddenischemic death. Eur Heart J 1989;10(3):203–8.
33] Falk E. Why do plaques rupture? Circulation 1992;86(Suppl.):30–42.34] Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Koletis GJ.
Compensatory enlargement of human atherosclerotic coronary arteries. NEngl J Med 1987;316:1371–5.
35] Schoenhagen P, Ziada KM, Kapadia SR, Crowe TD, Nissen SE, TuzcuEM. Extent and direction of arterial remodeling in stable versus unsta-ble coronary syndromes: an intravascular ultrasound study. Circulation2000;101:598–603.
36] Pasterkamp G, Schoneveld AH, van der Wal AC, Haudenschild CC, ClarijsRJ, Becker AE, et al. Relation of arterial geometry to luminal narrowingand histologic markers for plaque vulnerability: the remodeling paradox. JAm Coll Cardiol 1998;32:655–62.
37] Gyongyosi M, Yang P, Hassan A, Weidinger F, Domanovits H, LaggnerA, et al. Arterial remodelling of native human coronary arteries in patientswith unstable angina pectoris: a prospective intravascular ultrasound study.Heart 1999;82:68–74.
38] Moriushi M, Saito S, Honye J, Takaiwa Y, Ozawa Y, KanmatsuseK. Role of intravascular ultrasound imaging for assessing patho-physiology of coronary artery disease. J Cardiol 2000;35(Suppl.):51–5.
39] Smits PC, Pasterkamp G, de Jaegere PP, de Feyter PJ, Borst C. Angioscopiccomplex lesions are predominantly compensatory enlarged: an angioscopicand intracoronary ultrasound study. Cardiovasc Res 1999;41(2):458–64[460].



![Background and objective. arXiv:1810.13304v2 [cs.CV] 24 Apr 2019 · 2019. 4. 25. · arXiv:1810.13304v2 [cs.CV] 24 Apr 2019 Acute and sub-acute stroke lesion segmentation from multimodal](https://img.pdfslide.fr/doc/110x75/60c7a368e1068e57024b04ee/background-and-objective-arxiv181013304v2-cscv-24-apr-2019-2019-4-25.jpg)