Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Primary care physicians’ knowledge of the ophthalmic effectsof diabetesMichael N. Wiggins, MD,* Reid D. Landes, PhD,† Swetangi D. Bhaleeya, MD,*Sami H. Uwaydat, MD*
ABSTRACT ● RÉSUMÉ
Objective: Previous studies suggest that many patients with diabetes do not receive an annual dilated eye examination because of alack of referrals from primary care physicians (PCPs). This study aims to determine the depth of knowledge of PCPs regardingdiabetic eye disease.
Design: Cross-sectional assessment.Participants: Ninety-seven PCPs.Methods: An 8-question, multiple-choice assessment was administered over a 3-month period to 208 PCPs in attendance at
continuing medical education conferences.Results: Ninety-seven PCPs completed the assessment. Participants had a mean total score of 5.9 of 8 possible (73.8%).
Questions regarding screening, clinical findings, and prevention were answered correctly by ≥81% of the respondents. However,questions regarding risk factors and complications were answered correctly by less than 35% of the respondents. No difference inscores was found based on the type of residency training received or the number of years in practice.
Conclusions: Although PCPs may require greater education in the complications and risk factors of diabetic eye disease, studyparticipants demonstrated a good overall depth of knowledge regarding diabetic eye disease. Thus, previous reports of only 35%to 55% of patients with diabetes receiving an annual dilated fundus examination are likely not due to a lack of physician education.
Objet : Les études précédentes suggèrent que de nombreux patients diabétiques n'ont pas d'examen annuel du fond d'œil dilaté, àcause d'un manque de référence de la part des médecins de soins primaires (MSP). Cette étude vise à déterminer la profondeurdes connaissances des MSP concernant la maladie oculaire diabétique.
Nature : Évaluation transversale.Participants : Quatre-vingt-dix-sept MSP.Méthodes : À partir de 8 questions à choix multiples, l'on a évalué 208 MSP qui assistaient à des conférences de formation
médicale continue, sur une période de 3 mois.Résultats : Quatre-vingt-dix-sept MSP ont complété l'évaluation. Les participants avaient une moyenne globale de résultats de 5,9
sur une possibilité de 8 (73,8%). Parmi ceux-ci, ≥81% des répondants ont répondu correctement aux questions concernant ledépistage, les constatations cliniques et la prévention. Toutefois, moins de 35% ont répondu correctement aux questionsconcernant les facteurs de risque et les complications. Il n'y a pas eu de différence dans les résultats concernant le type deformation reçue en résidence ni le nombre d'années d'exercice.
Conclusions : Bien que les MSP aient peut-être besoin de plus de formation concernant les complications et les facteurs de risquede maladie oculaire chez les diabétiques, les participants à l'étude ont démontré un bon et profond savoir général concernant lamaladie oculaire diabétique. Ainsi, l'application, selon les rapports précédents, d'un examen annuel du fond d'œil dilaté àseulement 35% à 55% des patients diabétiques, n'était apparemment pas due à un manque de formation médicale.
Diabetic retinopathy is a leading cause of blindness in theUnited States among adults 24 to 75 years of age.1
Blindness from diabetes costs in the United States areapproximately US$500 million annually in lost incomeand associated services.2,3 Primary care physicians (PCPs)are the front-line caregivers for patients with diabetes andare the most important conveyors of information topatients regarding diabetic retinopathy. Therefore, under-standing the ocular manifestations of diabetes and know-ing the screening guidelines can impact the timeliness ofreferrals to ophthalmology by PCPs.4,5 It is well-known toophthalmologists that in proliferative diabetic retinopathy,
From the *Jones Eye Institute, University of Arkansas for MedicalSciences; and †Department of Biostatistics, University of Arkansas forMedical Sciences, Little Rock, AR
Originally received Dec. 8, 2011. Final revision Mar. 14, 2013. AcceptedMar. 26, 2013
Correspondence to Reid D. Landes, Department of Biostatistics, Uni-versity of Arkansas for Medical Sciences, 4301 West Markham Street,Slot 781, Little Rock, AR 72205-7199; [email protected]
C
the timing of the laser treatment can have a considerableeffect on the long-term vision of the patient.6,7 Properlydiagnosing diabetic retinopathy requires a dilated fundusexamination once or more per year. However, studies havereported that only 31% to 65% of patients with diabetesreceive an annual dilated fundus examination.4,8–14
Although this low rate is largely speculated to be due topatient misunderstanding and noncompliance, PCP refer-ral to an eye care specialist may also be a factor. Forinstance, Jacques et al.15 reported that only 72% of PCPssurveyed in Pennsylvania routinely refer their patients forvision care. Another study found that among family
Can J Ophthalmol 2013;48:265–2680008-4182/13/$-see front matter & 2013 Canadian OphthalmologicalSociety. Published by Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.jcjo.2013.03.011
AN J OPHTHALMOL—VOL. 48, NO. 4, AUGUST 2013 265
Ophthalmic effects in diabetes—Wiggins et al.
practice physicians, only 24% referred their pregnantpatients with preexisting diabetes to an ophthalmologist.16
This finding occurs at a time when the number of medicalschools requiring an ophthalmology rotation has signifi-cantly decreased from 68% in 2000 to 30% in 2004.17,18
With a minimal level of training and studies suggesting asuboptimal screening pattern, is the amount of educationand awareness concerning diabetic eye disease at issue? Asurvey of Canadian family physicians showed thatalthough 80% were aware of the screening guidelines fortype II diabetes, only 44% knew that diabetic women whobecome pregnant should be screened in the first trimesterfor retinopathy. Also, only one third of the physiciansknew that diabetic macular edema can present withoutvisual symptoms.19
Studies regarding awareness of diabetic eye diseaseamong PCPs have been performed in other coun-tries.11,20,21 However, little is known about the depth ofknowledge of U.S.-trained PCPs. Our study attempts tolearn more by asking the following questions: (i) Howmuch do PCPs know about the relationship betweendiabetes and eye care as it pertains to their practice?(ii) Are there gaps in the knowledge of diabetic retinop-athy (a) screening, (b) clinical findings and methods ofprevention, or (c) ocular complications and risk factors?(iii) Do any gaps depend on the type of training the PCPunderwent or on the PCP’s level of experience? Ouroverarching goals are to detect any deficiencies and providedirection for addressing any concerns.
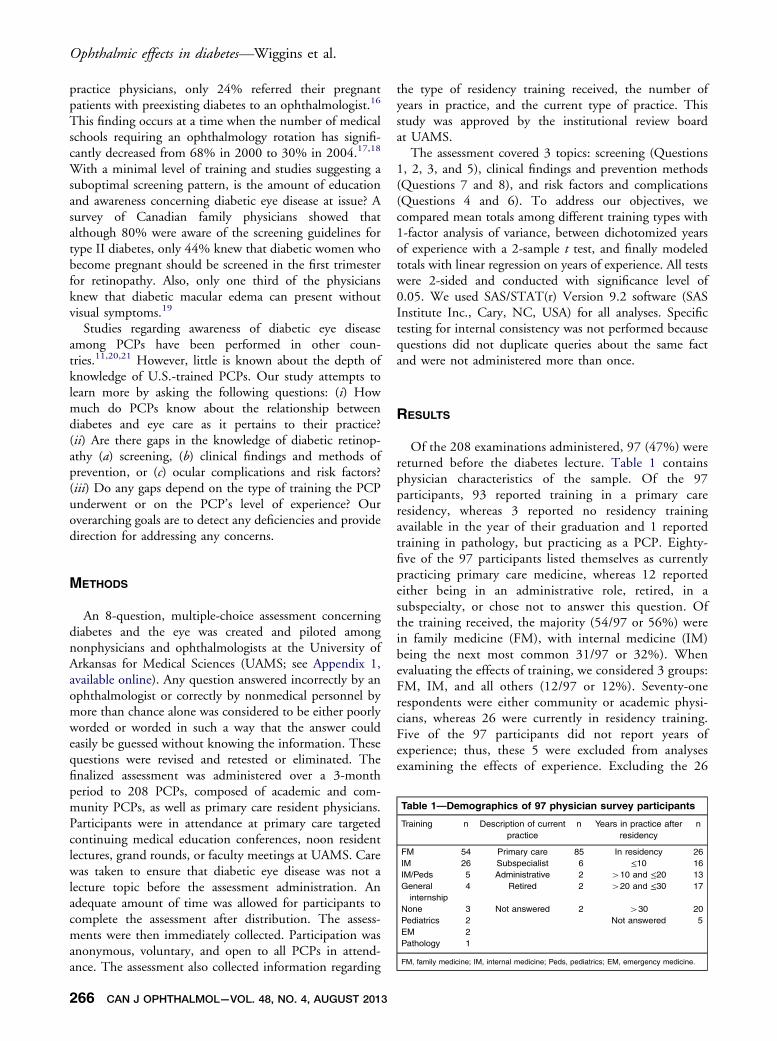
Table 1—Demographics of 97 physician survey participants
Training n Description of currentpractice
n Years in practice afterresidency
n
FM 54 Primary care 85 In residency 26IM 26 Subspecialist 6 ≤10 16IM/Peds 5 Administrative 2 410 and ≤20 13Generalinternship
4 Retired 2 420 and ≤30 17
None 3 Not answered 2 430 20Pediatrics 2 Not answered 5EM 2Pathology 1
FM, family medicine; IM, internal medicine; Peds, pediatrics; EM, emergency medicine.
METHODS
An 8-question, multiple-choice assessment concerningdiabetes and the eye was created and piloted amongnonphysicians and ophthalmologists at the University ofArkansas for Medical Sciences (UAMS; see Appendix 1,available online). Any question answered incorrectly by anophthalmologist or correctly by nonmedical personnel bymore than chance alone was considered to be either poorlyworded or worded in such a way that the answer couldeasily be guessed without knowing the information. Thesequestions were revised and retested or eliminated. Thefinalized assessment was administered over a 3-monthperiod to 208 PCPs, composed of academic and com-munity PCPs, as well as primary care resident physicians.Participants were in attendance at primary care targetedcontinuing medical education conferences, noon residentlectures, grand rounds, or faculty meetings at UAMS. Carewas taken to ensure that diabetic eye disease was not alecture topic before the assessment administration. Anadequate amount of time was allowed for participants tocomplete the assessment after distribution. The assess-ments were then immediately collected. Participation wasanonymous, voluntary, and open to all PCPs in attend-ance. The assessment also collected information regarding
266 CAN J OPHTHALMOL—VOL. 48, NO. 4, AUGUST 2013
the type of residency training received, the number ofyears in practice, and the current type of practice. Thisstudy was approved by the institutional review boardat UAMS.
The assessment covered 3 topics: screening (Questions1, 2, 3, and 5), clinical findings and prevention methods(Questions 7 and 8), and risk factors and complications(Questions 4 and 6). To address our objectives, wecompared mean totals among different training types with1-factor analysis of variance, between dichotomized yearsof experience with a 2-sample t test, and finally modeledtotals with linear regression on years of experience. All testswere 2-sided and conducted with significance level of0.05. We used SAS/STAT(r) Version 9.2 software (SASInstitute Inc., Cary, NC, USA) for all analyses. Specifictesting for internal consistency was not performed becausequestions did not duplicate queries about the same factand were not administered more than once.
RESULTS
Of the 208 examinations administered, 97 (47%) werereturned before the diabetes lecture. Table 1 containsphysician characteristics of the sample. Of the 97participants, 93 reported training in a primary careresidency, whereas 3 reported no residency trainingavailable in the year of their graduation and 1 reportedtraining in pathology, but practicing as a PCP. Eighty-five of the 97 participants listed themselves as currentlypracticing primary care medicine, whereas 12 reportedeither being in an administrative role, retired, in asubspecialty, or chose not to answer this question. Ofthe training received, the majority (54/97 or 56%) werein family medicine (FM), with internal medicine (IM)being the next most common 31/97 or 32%). Whenevaluating the effects of training, we considered 3 groups:FM, IM, and all others (12/97 or 12%). Seventy-onerespondents were either community or academic physi-cians, whereas 26 were currently in residency training.Five of the 97 participants did not report years ofexperience; thus, these 5 were excluded from analysesexamining the effects of experience. Excluding the 26

Table 2—Overall survey results of 97 physician participants, by topic
S All S correct CF P CF and P correct C R C and R correct
Question 1 2 3 5 — 7 8 — 4 6 —
Count (%) of Correct Responses 86 (89) 89 (92) 79 (81) 94 (97) 63 (65) 87 (90) 82 (85) 73 (75) 25 (26) 33 (34) 10 (10)
S, screening; CF, clinical findings; P, prevention; C, complications; R, risk factors.
Ophthalmic effects in diabetes—Wiggins et al.
residents (with 0 years experience), the average experi-ence was 23.3 years (SD 13.8 years, n ¼ 66). Althoughpractice location data were not addressed on the assess-ment, the type of conference attended (i.e., an academicfaculty meeting vs a community physician–targetedCME conference) suggested that 47 of the 97 partic-ipants practiced in the community, 36 participants(including 26 residents) were in an academic setting,and 14 could not be determined.
Participants had a mean total score of 5.9 (SD 1.0) outof 8 possible (73.8%). The means among the 3 trainingtypes ranged from 6.1 for FM-trained physicians to 5.9 forthose trained in IM to 5.6 for physicians trained in a fieldother than FM or IM, but did not statistically differ(F[2,94] ¼ 1.32, p ¼ 0.2725). Nor was there compellingevidence that total scores depended on experience,whether dichotomized into more or less than 10 years ofexperience (respective means of 6.0 vs 5.9; t[90] ¼ 0.35,p ¼ 0.7239) or when experience was treated as acontinuous variable (slope for an increase of 1 year¼ –0.002, t[90] ¼ 0.30, p ¼ 0.7678). Table 2 containsthe percent of correct answers for each question. Consid-ered individually, questions from the topics of screening(Questions 1, 2, 3, and 5) and clinical findings andprevention (Questions 7 and 8) were answered correctlyby ≥81% of the respondents. However, a large deficit inknowledge about risk factors and complications (Ques-tions 4 and 6) was clear, with less than 35% of therespondents answering either of these questions correctly.
DISCUSSION
Our study set out to learn why many diabetics may notbe getting proper ophthalmic care. Assuming the issuecould be physician education, physician compliance,patient communication, patient compliance, or anotherbarrier, we chose to begin the investigation by looking atphysician education; that is, the depth of knowledge ofPCPs regarding diabetic eye disease. We wanted toidentify any potential gaps of knowledge and to be ableto make recommendations to address any problemsidentified. To be able to adequately describe deficienciesand provide specific recommendations, we broke ourinvestigation down into specific areas in diabetic eye care:(i) screening, (ii) clinical findings and methods of pre-vention, and (iii) ocular complications and risk factors.Furthermore, we wanted to be able to provide information
C
regarding which PCPs might need additional education, ifdifferences among PCPs were found.
The strengths of our study include a good response ratefor a study of this design and a good cross section ofphysicians from the community and an academic setting.The sample also had a range of more than 50 years ofexperience. This wide range allowed us to investigate howknowledge might vary with experience. With an overallscore of 73.8%, the PCPs in our study had a good overalldepth of knowledge of diabetic eye disease.
We learned that participants scored poorly overall onQuestions 4 and 6 regarding complications and riskfactors. These findings suggest that greater education inthese areas may be needed for most PCPs. Alternatively, itis possible that the available choices for these 2 questionscould have influenced some of the incorrect responses.Questions 4 and 6 contained an item choice of “all of theabove.” This choice was not the correct answer for eitherquestion. It is possible that the temptation of choosing “allof the above” was too great for some participants.However, the assessment was well-piloted and did notidentify these 2 items as being confusing or poorly wordedin any way. In addition, physicians are intelligent, well-experienced test takers. It is therefore reasonable toconclude that some participants just did not know theinformation.
As our results are taken from physicians in the ruralsouthern United States, it is possible that PCPs in otherareas of the country might score differently. However,based on our varied cross section of private practice andacademic physicians of variable experience, our study islikely representative of many PCPs. Another potentialdrawback of our study is the small number of questionsgiven to participants. More assessment items could haveprovided more detailed data. However, as the partici-pants were voluntary and uncompensated, we believe amore labor-intensive assessment would have discouragedparticipation.
Given that complications of diabetic eye disease arelargely preventable when detected early and the largeamounts of resources that are spent annually in the UnitedStates to care for patients with diabetic complications, fewwould agree that the published reports of less than half ofdiabetic patients receiving adequate annual screening isacceptable. Our findings reveal that regardless of the typeof primary care training or the number of years ofexperience, PCPs are well educated in regard to diabeticeye disease. If our findings are generalizable to all PCPs,then the lack of examinations are likely due to an issue
AN J OPHTHALMOL—VOL. 48, NO. 4, AUGUST 2013 267

Ophthalmic effects in diabetes—Wiggins et al.
other than physician knowledge. Thus, other avenues ofinvestigation into the cause of this problem, such asexamining physician compliance, patient communication,patient compliance, or other barriers to health care need tobe explored.
Online-only material: This article includes online material.Appendix 1 can be found on the CJO web site at cos-sco.ca orcanadianjournalofophthalmology.ca. It is linked to this article inthe online contents of the August 2013 issue.Disclosure: The authors have no proprietary or commercial inte-rest in any materials discussed in this article.Supported By: This work was supported by unrestricted grantsfrom Research to Prevent Blindness and the Pat & WillardWalker Eye Research Center, and also by Award1UL1RR029884 from the National Center for ResearchResources.
REFERENCES
1. American Academy of Ophthalmology, Preferred practice pattern:diabetic retinopathy. San Francisco: Academy of Ophthalmology;1998.
2. Zhang X, Norris SL, Saadine J, Chowdhury FM, Horsley T, Kanjilal S,Mangione CM, Buhrmann R. Effectiveness of interventions to promotescreening for diabetic retinopathy. Am J Prev Med. 2007;33:318-35.
3. Klein R, Klein BEK. Vision disorders in diabetes. Diabetes inAmerica, 2nd ed. NIH publication no. 95-1448. Bethesda, Md.:National Institutes of Health, National Institute of Diabetes andDigestive and Kidney Diseases; 1995:293-338.
4. Sinclair SH, Delvecchio C. The internist’s role in managing diabeticretinopathy: screening for early detection. Cleve Clin J Med. 2004;71(2):151-9.
5. Paulus YM, Gariano RF. Diabetic retinopathy: a growing concern inan aging population. Geriatrics. 2009;64:16-26.
6. The Diabetic Retinopathy Study Research Group. Photocoagulationtreatment of proliferative diabetic retinopathy. Clinical applicationof Diabetic Retinopathy Study (DRS) findings, DRS report number8. Ophthalmology. 1981;88:583-600.
7. Chew EY, Ferris FL 3rd, Csaky KG, et al. The long-term effects oflaser photocoagulation in patients with diabetic retinopathy: the
268 CAN J OPHTHALMOL—VOL. 48, NO. 4, AUGUST 2013
early treatment diabetic retinopathy follow-up study. Ophthalmology.2003;110:1683-9.
8. Wang F, Javitt JC. Eye care for elderly Americans with diabetesmellitus. Failure to meet current guidelines. Ophthalmology.1996;103:1744-50.
9. Mukamel DB, Bresnick GH, Wang Q, Dickey CF. Barriers tocompliance with screening guidelines for diabetic retinopathy.Ophthalmic Epidemiol. 1999;6:61-72.
10. Weiner JP, Parente ST, Garnick DW, Fowles J, Lawthers AG,Palmer RH. Variation in office-based quality: a claim-based profileof care provided to Medicare patients with diabetes. JAMA.1995;273:1503-8.
11. Nguyen TT, Daniels NA, Gildengorin G, Perez-Stable EJ. Eth-nicity, language, specialty care, and quality of diabetes care. EthnDis. 2007;17:65-71.
12. Schoenfeld E, Greene JM, Wu SY, Leske C. Patterns of adherenceto diabetes vision care guidelines: baseline findings from theDiabetic Retinopathy Awareness Program. Ophthalmology.2001;108:563-71.
13. Brechner RJ, Cowie CC, Howie LJ, Herman WH, Will JC, HarrisMI. Ophthalmic examination among adults with diagnosed diabetesmellitus. JAMA. 1993;270:1714-8.
14. Moss SE, Klein R, Klein BE. Factors associated with having eyeexaminations in persons with diabetes. Arch Fam Med.1995;4:529-34.
15. Jacques CHM, Jones RL, Houts P, et al. Reported practice behaviorsfor medical care of patients with diabetes mellitus by primary-carephysicians in Pennsylvania. Diabetes Care. 1991;14:712-7.
16. Marrero DG, Moore PS, Langefeld CD, Clark CM Jr. Patterns ofreferral and examination for retinopathy in pregnant women withdiabetes by primary care physicians. Ophthalmic Epidemiol.1995;2:93-8.
17. Higginbotham EJ, Rust G. Ophthalmology and primary care:partners in peril? Arch Ophthalmol. 2008;126:727-8.
18. Quillen DA, Harper RA, Haik BG. Medical student education inophthalmology: crisis and opportunity. Ophthalmology. 2005;112:1867-8.
19. Delorme C, Boisjoly HM, Baillargeon L, Turcotte P, Bernard PM.Screening for diabetic retinopathy. Do family physicians know theCanadian guidelines? Can Fam Phys. 1998;44:1473-9.
20. Preti RC, Saraiva F, Junior JA, Takahashi WY, da Silva ME. Howmuch information do medical practitioners and endocrinologistshave about diabetic retinopathy? Clinics (Sao Paulo). 2007;62:273-8.
21. Muecke JS, Newland HS, Ryan P, et al. Awareness of diabetic eyedisease among general practitioners and diabetic patients in Yangon,Myanmar. Clin Experiment Ophthalmol. 2008;36:265-73.