Embed Size (px)
Citation preview

TRITON : Quel bénéfice clinique ?
Dr François PHILIPPEInstitut Mutualiste Montsouris
Paris

Modified from Storey Platelets 12: 197, 2001
HOOCHOOCHOOCHOOC
* HSHS* HSHS
NNNN
OOOO
FFFF
P2Y12P2Y1P2X1
Active MetaboliteActive Metabolite of Prasugrel of Prasugrel
Inhibition des récepteurs purinegiques

0
100
200
300
400
500
600
AUC
0
100
200
300
400
500
600
Cmax
0
10
20
30
40
50
60
70
Tmax
Payne et al, ISTH, 2005ng/ml
Minutes
ng*hr/ml
Niveaux des métabolites actifsNiveaux des métabolites actifs
Prasugrel 60mgClopidogrel 300mg
Time from Dose (hr)
0 6 12 18 24
Pla
sma
Con
cent
ratio
n (n
g/m
L)
0
100
200
300
400
500
600
300 mg Clopidogrel
60 mg Prasugrel

Inhibition de l’aggrégation plaquettaire à 2 heuresInhibition de l’aggrégation plaquettaire à 2 heures
Moindre variabilitéMoindre variabilité
Individual IPA to 20 μM ADP 2 hr after LD
Variance for prasugrel p<0.01 vs. either clopidogrel groupIn
hib
itio
n o
f P
late
let
Ag
gre
gat
ion
(%
)
-20
0
20
40
60
80
100
CLOP300 mg LD
CLOP600 mg LD
PRAS60 mg LD
Clop 300/75
Clop 600/75
Pras 60/10

Inhibition de l’aggrégation plaquettaireInhibition de l’aggrégation plaquettaire
Après dose de charge : précocité et puissanceAprès dose de charge : précocité et puissance
mean ± SEM 20 μM ADP
Temps après dose de charge (hrs)
Inh
ibit
ion
of
Pla
tele
t A
gg
reg
ati
on
(%
)
0
20
40
60
80
100
Clop 300 mg LD
0.25 0.5 1 2 4 6 24
Dose de charge
†p<0.001 vs. Clop 300
† †
!†
p<0.05 vs. Clop 300
!
Clop 600 mg LD
!
*
*
** * *
*p<0.001 vs. Clop 300 mgor 600 mg LD
Pras 60mg LD
0

Inhibition de l’aggrégation plaquettaireInhibition de l’aggrégation plaquettaire
Avec dose d’entretien : stabilitéAvec dose d’entretien : stabilité
mean ± SEM 20 μM ADP
Inh
ibit
ion
of
Pla
tele
t A
gg
reg
ati
on
(%
)
0
20
40
60
80
100
Dose de charge Dose d’entretien
Temps Heures Jours
0.25 0.5 1 2 4 6 24 3 4 5 6 7 8 90
Clop 300 mg
Clop 75 mg
††
!
!
† §
†p<0.001 vs. Clop 300
!p<0.05 vs. Clop 300§p<0.05 vs Clop 300/75
Clop 600 mg
Clop 75 mg
*
*
** * *
* * * * * * *
*p<0.001 vs. Clop 300 mg or 600 mg LD
Pras 60 mg
Pras 10 mg

TRial to Assess Improvement in Therapeutic
Outcomes by Optimizing Platelet InhibitioN with
Prasugrel
TRITON-TIMI 38TRITON-TIMI 38AHA 2007AHA 2007
Orlando, FloridaOrlando, Florida

Hypothèse principale : SUPERIORITEHypothèse principale : SUPERIORITE
Prasugrel + ASA > clopidogrel + ASA
pour la prévention des événements cliniques chez des patients avec SCA, à risque modéré
et élevé, subissant une angioplastie
Première étude d’envergure testant l’hypothèse qu’un inhibition plaquettaire plus intense et de moindre
variabilité puisse améliorer le pronostic des patients

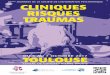
Schéma de l’étude
Double-blind
ACS (STEMI or UA/NSTEMI) & Planned PCI
ASA
PRASUGREL60 mg LD/ 10 mg MD
CLOPIDOGREL300 mg LD/ 75 mg MD
Critère principal : Décès CV, IDM, AVCCritères secondaires : Décès CV, IDM, AVC,
Réhospitalisation récidive isch., Thrombose de stent
Etudes ancillaires: Pharmacocinetique, génétique
Median duration of therapy - 12 months
N= 13,600

Caracteristiques basalesCaracteristiques basales

Procédure d’angioplastieProcédure d’angioplastie

RésultatsRésultats
Wiviott S et al. NEJM 2007;357:1999-2013

Slides and Full Listing of Trial Participants at www.TIMI.orgSlides and Full Listing of Trial Participants at www.TIMI.org
www.NEJM.orgwww.NEJM.org

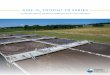
EfficacitéEfficacité
Wiviott S et al. NEJM 2007;357:1999-2013

0
5
10
15
0 30 60 90 180 270 360 450
HR 0.81(0.73-0.90)P=0.0004
Prasugrel
Clopidogrel
Days
En
dp
oin
t (%
)
12.1
9.9
138 events
Crière principal – Population globaleCrière principal – Population globale
CV Death / MI / Stroke
NNT = 46N=643
N=781

Chronologie du bénéficeChronologie du bénéfice(Landmark Analysis - 3 days)(Landmark Analysis - 3 days)
Pri
ma
ry E
nd
po
int
(%)

SécuritéSécurité
Wiviott S et al. NEJM 2007;357:1999-2013

Saignements majeurs hors PACSaignements majeurs hors PAC

Evénements hémorragiquesEvénements hémorragiques(N=13 457)(N=13 457)
% E
ven
ts%
Eve
nts
ARD 0.6%ARD 0.6%HR 1.32HR 1.32P=0.03P=0.03
NNH=167 NNH=167
ARD 0.5%ARD 0.5%HR 1.52HR 1.52P=0.01P=0.01
ARD 0.2%ARD 0.2%P=0.23P=0.23
ARD 0%ARD 0%P=0.74P=0.74
ARD 0.3%ARD 0.3%P=0.002P=0.002
ICH in Pts w ICH in Pts w Prior Stroke/TIA Prior Stroke/TIA
(N=518)(N=518)
Clop 0 (0) %Clop 0 (0) % Pras 6 (2.3)%Pras 6 (2.3)% (P=0.02) (P=0.02)
1,8
0,9 0,9
0,10,3
2,4
1,41,1
0,4 0,3
0
2
4
TIMI MajorBleeds
LifeThreatening
Nonfatal Fatal ICH
ClopidogrelPrasugrel

Balance du bénéfice/risque
Bénéfice clinique net

Bénéfice clinique netBénéfice clinique net
Décès, IDM, AVC, Saignement majeurDécès, IDM, AVC, Saignement majeur
0
5
10
15
0 30 60 90 180 270 360 450Days
En
dp
oin
t (%
)
HR 0.87P=0.004
13.9
12.2
Prasugrel
Clopidogrel
109 events
ITT= 13,608ITT= 13,608
-23
6
-25
-20
-15
-10
-5
0
5
10
Events per 1000 ptsEvents per 1000 pts
MIMI Major BleedMajor Bleed(non CABG)(non CABG)
++All CauseAll CauseMortalityMortality
Clop 3.2%Clop 3.2%Pras 3.0 %Pras 3.0 %
P=0.64P=0.64

Benéfice clinique netBenéfice clinique net Sous-groupes à haut risque hémorragiqueSous-groupes à haut risque hémorragique
Total
>=60 kg
< 60 kg
< 75
> 75
No
Yes
0.5 1 2
ATCDAVC/AIT
Age
Poids
Risk (%)
+ 37
-16
-1
-16
+3
-14
-13
Prasugrel Better Clopidogrel BetterHR
Pint = 0.006
Pint = 0.18
Pint = 0.36
Post-hoc analysisPost-hoc analysis

Prévention Prévention de la thrombose de stentde la thrombose de stent

Thrombose de stentThrombose de stent(ARC certaine + probable)(ARC certaine + probable)
0
1
2
3
0 30 60 90 180 270 360 450
HR 0.48P <0.0001
Prasugrel
Clopidogrel2.4
(142)
74 events
NNT= 77
1.1 (68)
Days
En
dp
oin
t (%
)
Any Stent at Index PCIAny Stent at Index PCI N= 12,844 N= 12,844
Kaplan-Meier estimates of the incidence of definite or probable stent thrombosis—CEC adjudicatedKaplan-Meier estimates of the incidence of definite or probable stent thrombosis—CEC adjudicatedAll randomized All ACS subjects.All randomized All ACS subjects.

Chronologie de la prévention Chronologie de la prévention de la thrombose de stent de la thrombose de stent
(Landmark Analysis - 3 days) (Landmark Analysis - 3 days)

Patients diabétiquesPatients diabétiques
N = 3 146N = 3 146

Sous-groupe des diabétiquesSous-groupe des diabétiques
0
2
4
6
8
10
12
14
16
18
0 30 60 90 180 270 360 450
HR 0.70P<0.001
Days
En
dp
oin
t (%
) 68 events
CV Death / MI / Stroke
TIMI Major NonCABG Bleeds
NNT = 46
N = 3 146N = 3 146
17.0
12.2
Prasugrel
Clopidogrel
Prasugrel
Clopidogrel 2.6
2.5

Patients SCA ST +Patients SCA ST +
For internal use only - not for external use or promotion

TRITON TIMI-38 – Cohorte SCA ST +TRITON TIMI-38 – Cohorte SCA ST +
0
5
10
15
0 50 100 150 200 250 300 350 400 450
Pe
rce
nt
(%)
Days From Randomization
9.5%
6.5%
HR 0.68(0.54-0.87)
P=0.002
12.4%
10.0%
HR 0.79(0.65-0.97)
P=0.02
Clopidogrel
Prasugrel
For internal use only - not for external use or promotion
Primary endpoint: CV death, nonfatal MI, nonfatal stroke
Montalescot G, et al. Prasugrel compared with Clopidogrel in Patients Undregoing Percutaneous Coronary Intervention for ST-Elevation Myocardial Infarction in TRITON-TIMI 38. ESC 2008 Eur Heart J . 2008: 29 :334.
RRR 21%
NNT 42
Age adjusted HR 0.81 (0.66-0.99)

TRITON TIMI-38 – Cohorte SCA ST + TRITON TIMI-38 – Cohorte SCA ST + Thrombose de stent Thrombose de stent
0
0.5
1
1.5
2
2.5
3
0 50 100 150 200 250 300 350 400 450
Pe
rce
nt
(%)
Days from Randomization
2.4%
1.2%
HR 0.49(0.28-0.84)
P=0.008
HR 0.58(0.36-0.93)
P=0.008
2.8%
1.6%
Clopidogrel
Prasugrel
RRR 42%
NNT = 83
P=0.02
Age adjusted HR = 0.59, CI 95% 0.37-0.96
Montalescot G, et al. Prasugrel compared with Clopidogrel in Patients Undregoing Percutaneous Coronary Intervention for ST-Elevation Myocardial Infarction in TRITON-TIMI 38. ESC 2008 Eur Heart J . 2008: 29 :334.
For internal use only - not for external use or promotion

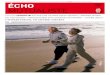
TRITON TIMI-38 - Cohorte SCA ST +TRITON TIMI-38 - Cohorte SCA ST +Hémorragies majeures TIMIHémorragies majeures TIMI
0
0.5
1
1.5
2
2.5
0 50 100 150 200 250 300 350 400 450
Per
cen
t (%
)
Days from Randomization
2.4%
2.1%
HR 1.11(0.70-1.77)
P=0.65
Clopidogrel
Prasugrel
Mai
n sa
fety
end
poin
t (T
IMI m
ajor
non
-C
AB
G b
leed
ings
)
All
ST
EM
I pat
ient
s
Montalescot G, et al. Prasugrel compared with Clopidogrel in Patients Undregoing Percutaneous Coronary Intervention for ST-Elevation Myocardial Infarction in TRITON-TIMI 38. ESC 2008 Eur Heart J . 2008: 29 :334.
For internal use only - not for external use or promotion

CONCLUSIONCONCLUSION
Hypothèse de supériorité validée (prasugrel > clopidogrel)
Un bénéfice clinique net (balance bénéfice/risque)
Une prévention accrue de la thrombose de stent
Identifier les sous-groupes à risque hémorragique élevé - ATCD AVC/AIT- > 75 ans- < 60 kg
Connaître les sous-groupes à balance très favorable- SCA ST +- diabétiques